

Effectiveness of self-managed medication abortion with accompaniment support in Argentina and Nigeria (SAFE): a prospective, observational cohort study and non-inferiority analysis with historical controls
- PMID: 34801131
- PMCID: PMC9359894
- DOI: 10.1016/S2214-109X(21)00461-7
Effectiveness of self-managed medication abortion with accompaniment support in Argentina and Nigeria (SAFE): a prospective, observational cohort study and non-inferiority analysis with historical controls
Abstract
Background: Clinical trials have established the high effectiveness and safety of medication abortion in clinical settings. However, barriers to clinical abortion care have shifted most medication abortion use to out-of-clinic settings, especially in the context of the COVID-19 pandemic. Given this shift, we aimed to estimate the effectiveness of self-managed medication abortion (medication abortion without clinical support), and to compare it to effectiveness of clinician-managed medication abortion.
Methods: For this prospective, observational cohort study, we recruited callers from two safe abortion accompaniment groups in Argentina and Nigeria who requested information on self-managed medication abortion. Before using one of two medication regimens (misoprostol alone or in combination with mifepristone), participants completed a baseline survey, and then two follow-up phone surveys at 1 week and 3 weeks after taking pills. The primary outcome was the proportion of participants reporting a complete abortion without surgical intervention. Legal restrictions precluded enrolment of a concurrent clinical control group; thus, a non-inferiority analysis compared abortion completion among those in our self-managed medication abortion cohort with abortion completion reported in historical clinical trials using the same medication regimens, restricted to participants with pregnancies of less than 9 weeks' gestation. This study was registered with ISCRTN, ISRCTN95769543.
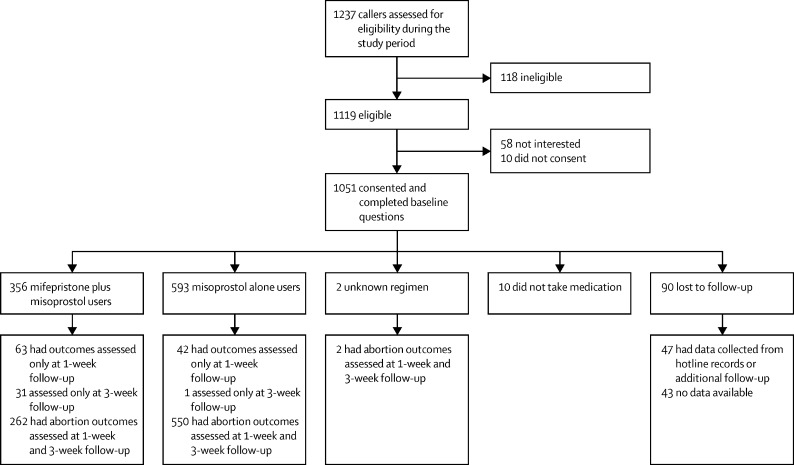
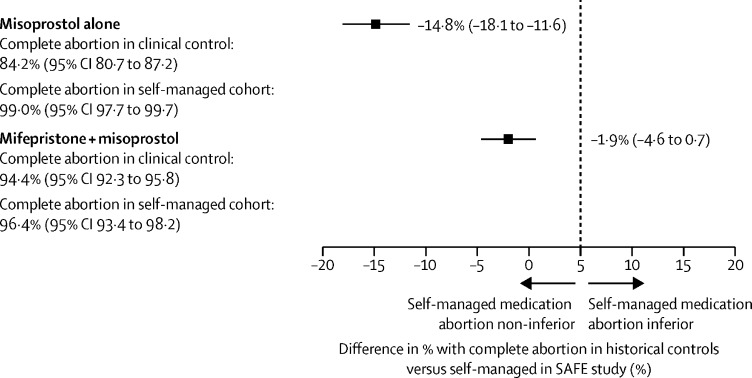
Findings: Between July 31, 2019, and April 27, 2020, we enrolled 1051 participants. We analysed abortion outcomes for 961 participants, with an additional 47 participants reached after the study period. Most pregnancies were less than 12 weeks' duration. Participants in follow-up self-managed their abortions using misoprostol alone (593 participants) or the combined regimen of misoprostol plus mifepristone (356 participants). At last follow-up, 586 (99%) misoprostol alone users and 334 (94%) combined regimen users had a complete abortion without surgical intervention. For those with pregnancies of less than 9 weeks' gestation, both regimens were non-inferior to medication abortion effectiveness in clinical settings.
Interpretation: Findings from this prospective cohort study show that self-managed medication abortion with accompaniment group support is highly effective and, for those with pregnancies of less than 9 weeks' gestation, non-inferior to the effectiveness of clinician-managed medication abortion administered in a clinical setting. These findings support the use of remote self-managed models of early abortion care, as well as telemedicine, as is being considered in several countries because of the COVID-19 pandemic.
Funding: David and Lucile Packard Foundation.
Translations: For the Arabic, French, Bahasa Indonesian, Spanish and Yoruba translations of the Article see Supplementary Materials section.
Copyright © 2022 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests We declare no competing interests.
Figures
References
-
- WHO . World Health Organization; Geneva: 2018. Medical management of abortion. - PubMed
-
- Rodriguez MI, Seuc A, Kapp N, et al. Acceptability of misoprostol-only medical termination of pregnancy compared with vacuum aspiration: an international, multicentre trial. BJOG. 2012;119:817–823. - PubMed
-
- Winikoff B, Sivin I, Coyaji KJ, et al. Safety, efficacy, and acceptability of medical abortion in China, Cuba, and India: a comparative trial of mifepristone-misoprostol versus surgical abortion. Am J Obstet Gynecol. 1997;176:431–437. - PubMed
-
- Chen MJ, Creinin MD. Mifepristone with buccal misoprostol for medical abortion: a systematic review. Obstet Gynecol. 2015;126:12–21. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
