

Mean Versus Peak Coronary Calcium Density on Non-Contrast CT: Calcium Scoring and ASCVD Risk Prediction
- PMID: 34801452
- PMCID: PMC8917973
- DOI: 10.1016/j.jcmg.2021.09.018
Mean Versus Peak Coronary Calcium Density on Non-Contrast CT: Calcium Scoring and ASCVD Risk Prediction
Abstract
Objectives: This study sought to assess the relationship between mean vs peak calcified plaque density and their impact on calculating coronary artery calcium (CAC) scores and to compare the corresponding differential prediction of atherosclerotic cardiovascular disease (ASCVD) and coronary heart disease (CHD) mortality.
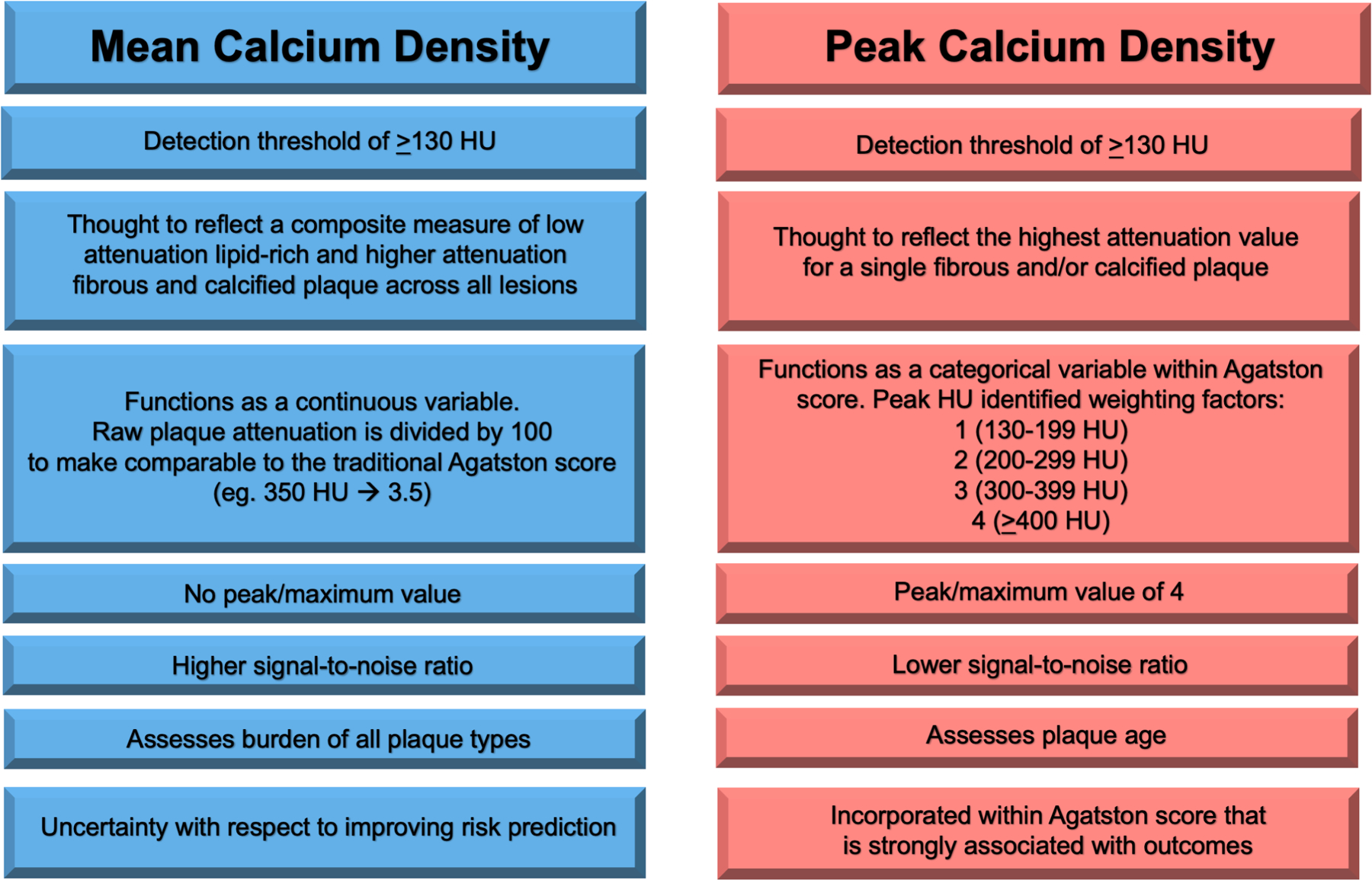
Background: The Agatston CAC score is quantified per lesion as the product of plaque area and a 4-level categorical peak calcium density factor. However, mean calcium density may more accurately measure the heterogenous mixture of lipid-rich, fibrous, and calcified plaque reflective of ASCVD risk.
Methods: We included 10,373 individuals from the CAC Consortium who had CAC >0 and per-vessel measurements of peak calcium density factor and mean calcium density. Area under the curve and continuous net reclassification improvement analyses were performed for CHD and ASCVD mortality to compare the predictive abilities of mean calcium density vs peak calcium density factor when calculating the Agatston CAC score.
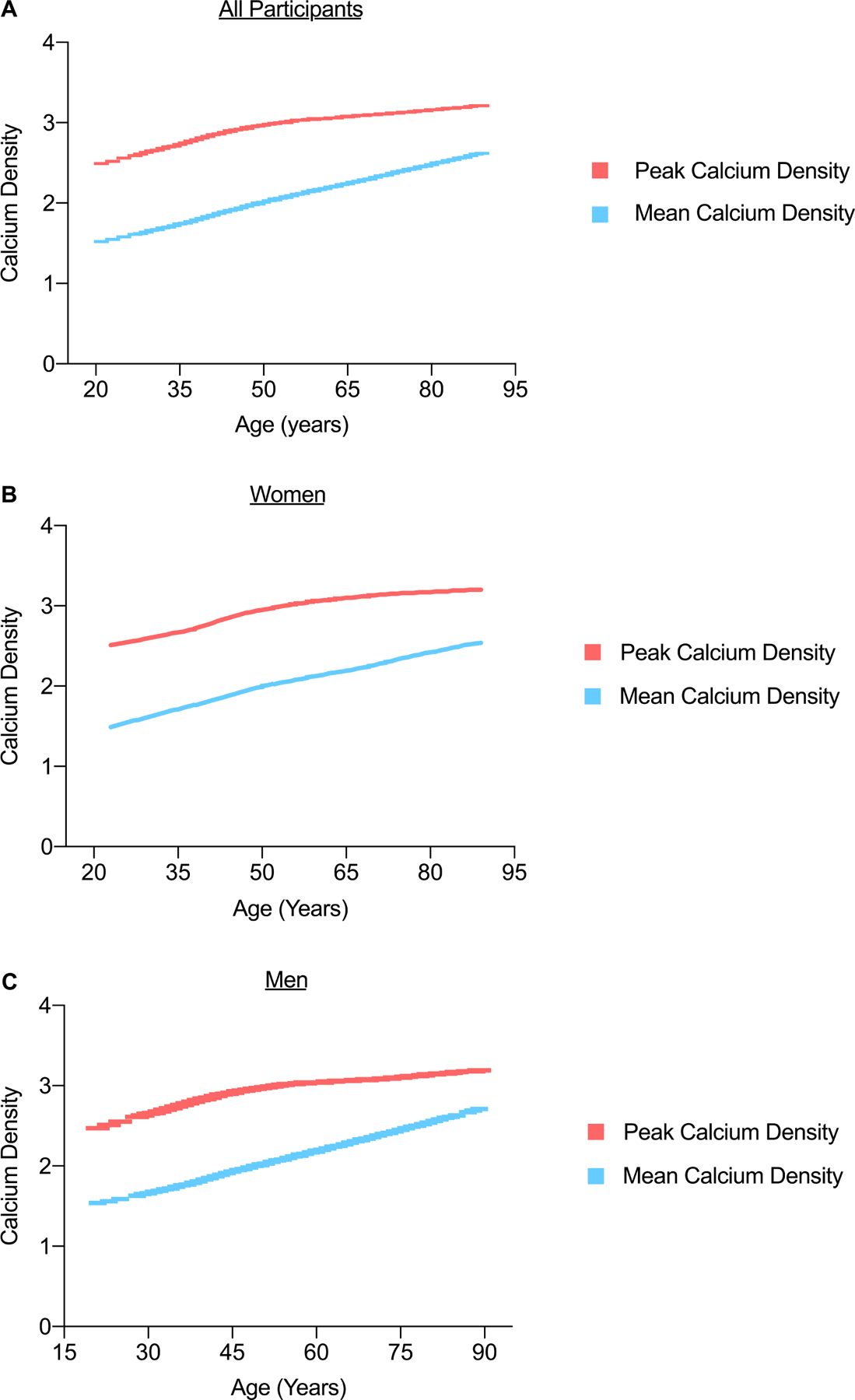
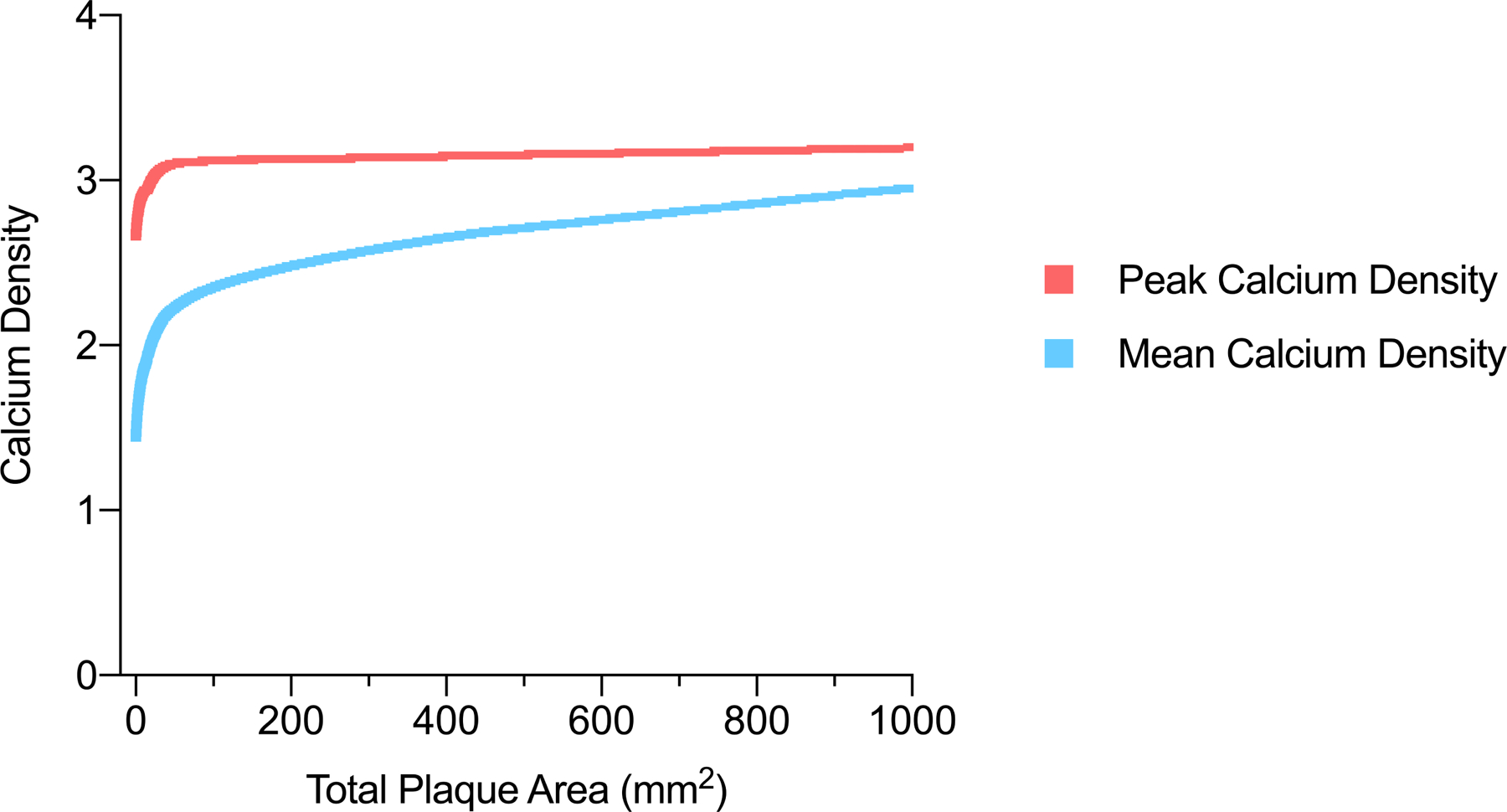
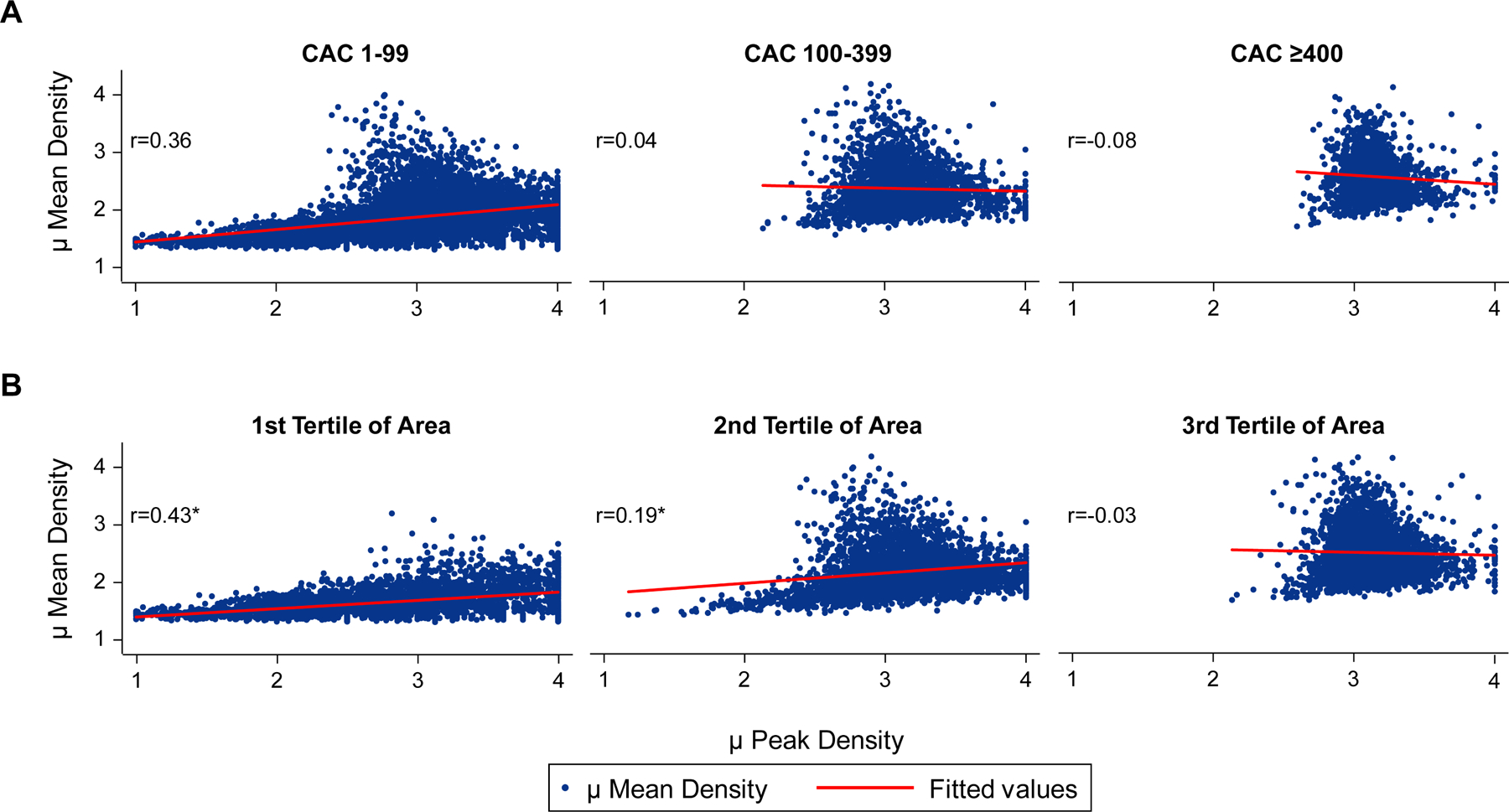
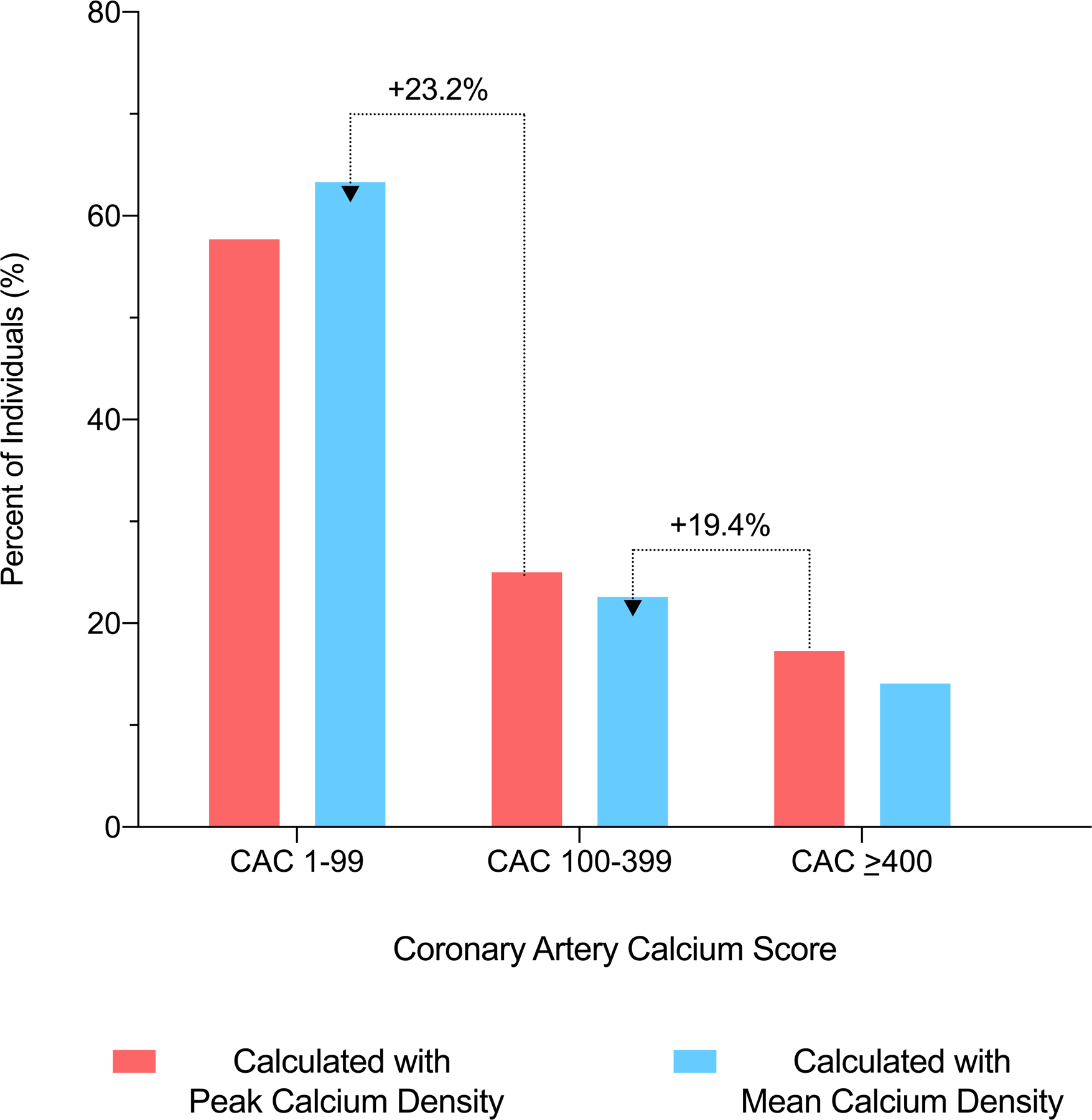
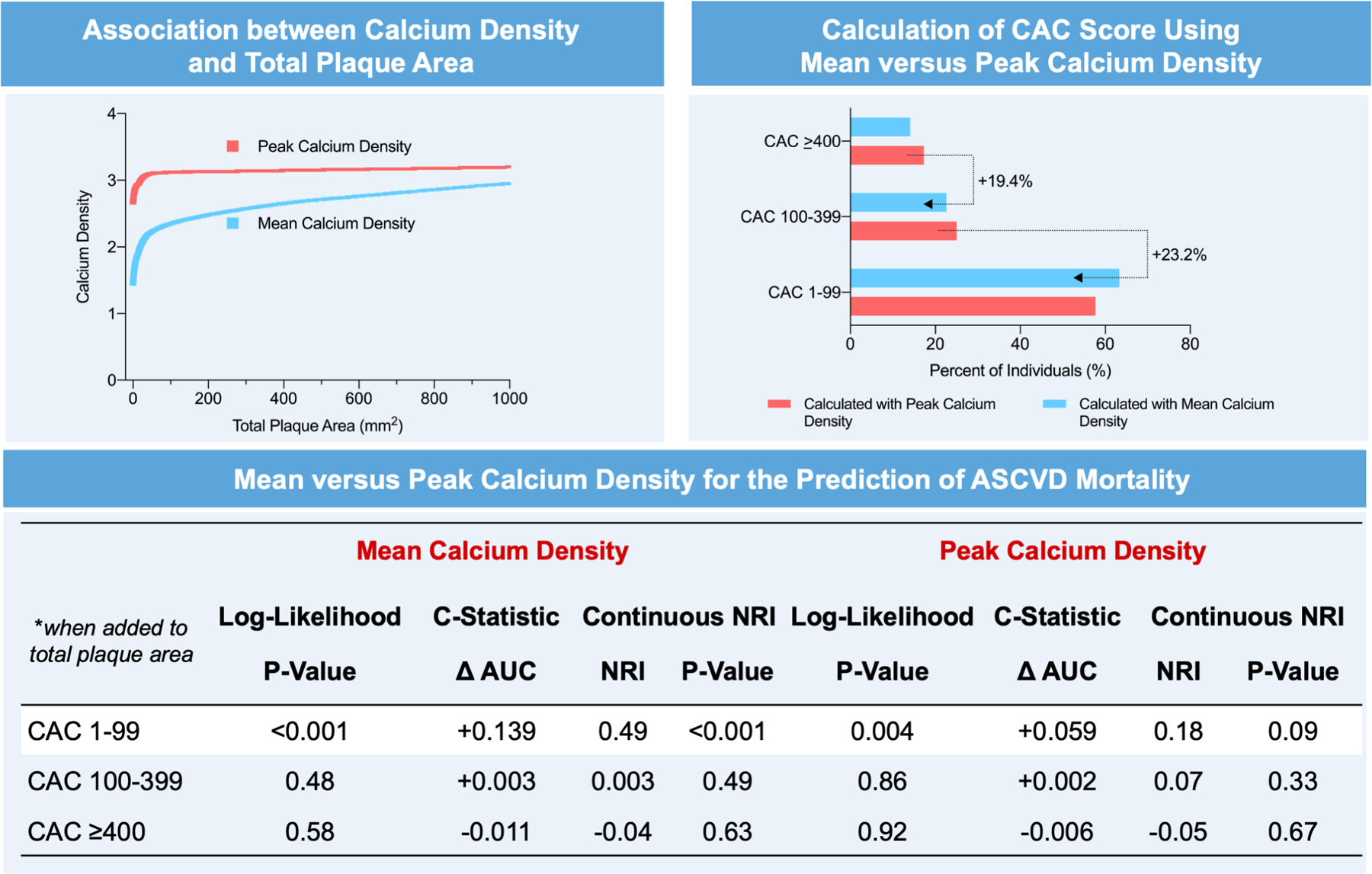
Results: Participants were on average 53.4 years of age, 24.4% were women, and the median CAC score was 68 Agatston units. The average values for mean calcium density and peak calcium density factor were 210 ± 50 HU and 3.1 ± 0.5, respectively. Individuals younger than 50 years of age and/or those with a total plaque area <100 mm2 had the largest differences between the peak and mean density measures. Among persons with CAC 1-99, the use of mean calcium density resulted in a larger improvement in ASCVD mortality net reclassification improvement (NRI) (NRI = 0.49; P < 0.001 vs. NRI = 0.18; P = 0.08) and CHD mortality discrimination (Δ area under the curve (AUC) = +0.169 vs +0.036; P < 0.001) compared with peak calcium density factor. Neither peak nor mean calcium density improved mortality prediction at CAC scores >100.
Conclusion: Mean and peak calcium density may differentially describe plaque composition early in the atherosclerotic process. Mean calcium density performs better than peak calcium density factor when combined with plaque area for ASCVD mortality prediction among persons with Agatston CAC 1-99.
Keywords: atherosclerotic plaque; calcium density; cardiovascular disease; coronary artery calcium; multidetector computed tomography; primary prevention; risk; vascular calcification.
Copyright © 2022 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures This project was supported in part by a research grant from the National Institutes of Health–National Heart, Lung, and Blood Institute (L30 HL110027). Dr Blaha has received grants from the National Institutes of Health, U.S. Food and Drug Administration, American Heart Association, and Aetna Foundation; grants and personal fees from Amgen; and personal fees from Sanofi, Regeneron, Novartis, Bayer, and Novo Nordisk outside the submitted work. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Comment in
-
How Should We Measure and Score Coronary Artery Calcium?JACC Cardiovasc Imaging. 2022 Mar;15(3):501-503. doi: 10.1016/j.jcmg.2021.11.004. Epub 2021 Dec 15. JACC Cardiovasc Imaging. 2022. PMID: 34922868 No abstract available.
References
-
- Agatston AS, Janowitz WR, Hildner FJ, Zusmer NR, Viamonte M, Detrano R. Quantification of coronary artery calcium using ultrafast computed tomography. J Am Coll Cardiol. 1990. Mar 15;15(4):827–32. - PubMed
-
- Virmani R, Burke AP, Farb A, Kolodgie FD. Pathology of the Vulnerable Plaque. Journal of the American College of Cardiology. 2006. - PubMed
-
- Blaha MJ, Mortensen MB, Kianoush S, Tota-Maharaj R, Cainzos-Achirica M. Coronary Artery Calcium Scoring: Is It Time for a Change in Methodology? JACC: Cardiovascular Imaging. 2017. - PubMed
-
- Zaromytidou M, Antoniadis AP, Siasos G, Coskun AU, Andreou I, Papafaklis MI, et al. Heterogeneity of Coronary Plaque Morphology and Natural History: Current Understanding and Clinical Significance. Current Atherosclerosis Reports. 2016. - PubMed
