

Spontaneous Upbeat Nystagmus and Selective Anterior Semicircular Canal Hypofunction on Video Head Impulse Test: A New Variant of Canalith Jam?
- PMID: 34802218
- PMCID: PMC9271735
- DOI: 10.7874/jao.2021.00297
Spontaneous Upbeat Nystagmus and Selective Anterior Semicircular Canal Hypofunction on Video Head Impulse Test: A New Variant of Canalith Jam?
Abstract
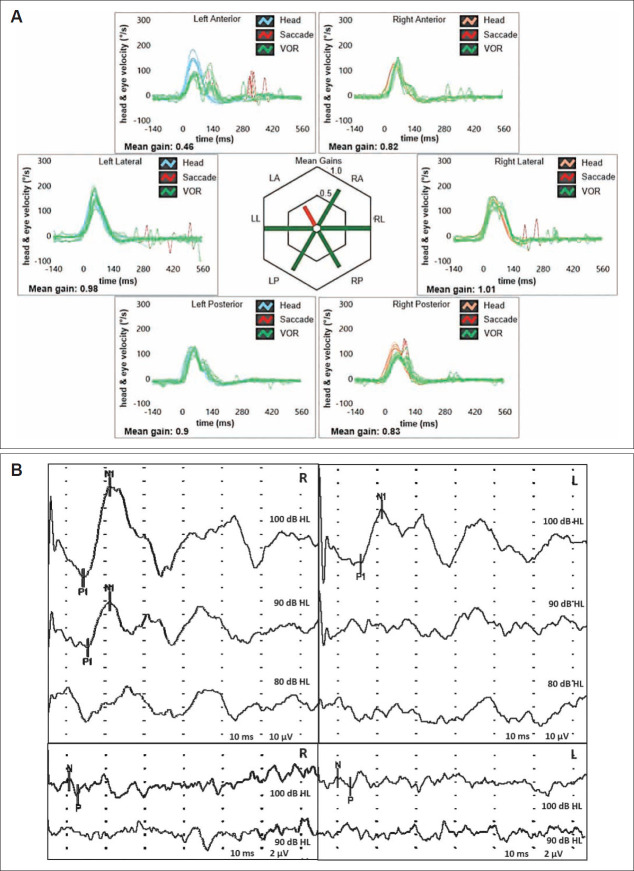
We describe a rare case of spontaneous upbeat nystagmus (UBN) attributable to a canalith jam involving the anterior semicircular canal (ASC) in a patient in whom comprehensive vestibular assessment was useful to identify the underlying pathomechanism. A 56-year-old woman with unsteadiness following repositioning procedures for left-sided benign paroxysmal positional vertigo (BPPV) presented with spontaneous UBN that showed slight right torsional components. A vestibular test battery detected isolated left ASC hypofunction on a video-head impulse test (Video-HIT). We postulated a persistent utriculopetal deflection of the left ASC cupula, which was attributable to entrapment of debris in a narrow canal tract, with consequent sustained inhibition of the ampullary afferents. Although spontaneous UBN receded after impulsive physical therapy, unsteadiness deteriorated into positional vertigo secondary to canalolithiasis involving the ipsilateral posterior canal. In our view, physical therapy possibly fragmented the canalith jam and released free-floating otoconia that eventually settled into the ipsilateral posterior canal. Video HIT revealed normalization of ASC hypofunction, and leftsided posterior canal canalolithiasis was successfully treated using appropriate repositioning procedures. We propose that a canalith jam involving the ASC should be considered in the differential diagnosis of spontaneous UBN, particularly in patients with a history of BPPV and isolated ASC hypofunction detected on video HIT.
Keywords: Benign paroxysmal positional vertigo; Head impulse test; Otoconia; Semicircular canals; Vertical nystagmus.
Figures


References
-
- Leigh RJ, Zee DS. The neurology of eye movements. 5th ed. New York: Oxford University Press; 2015.
-
- Reynard P, Karkas A, Gavid M, Lelonge Y, Bertholon P. Eur Ann Otorhinolaryngol Head Neck Dis. 2018;135:321–26. - PubMed
-
- Young AS, Lechner C, Bradshaw AP, MacDougall HG, Black DA, Halmagyi GM, et al. Capturing acute vertigo: a vestibular event monitor. Neurology. 2019;92:e2743–53. - PubMed
-
- Ko KM, Song MH, Kim JH, Shim DB. Persistent spontaneous nystagmus following a canalith repositioning procedure in horizontal semicircular canal benign paroxysmal positional vertigo. JAMA Otolaryngol Head Neck Surg. 2014;140:250–2. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
