

Adjuvant Chemotherapy for Muscle-invasive Bladder Cancer: A Systematic Review and Meta-analysis of Individual Participant Data from Randomised Controlled Trials
- PMID: 34802798
- PMCID: PMC8708165
- DOI: 10.1016/j.eururo.2021.09.028
Adjuvant Chemotherapy for Muscle-invasive Bladder Cancer: A Systematic Review and Meta-analysis of Individual Participant Data from Randomised Controlled Trials
Abstract
Context: Our prior systematic review and meta-analysis of individual participant data (IPD) suggesting a benefit of adjuvant chemotherapy for muscle-invasive bladder cancer was limited by the number and size of included randomised trials. We have updated results to include additional trials, providing the most up-to-date and reliable evidence of the effects of this treatment.
Objective: To investigate the role of adjuvant cisplatin-based chemotherapy in the treatment of muscle-invasive bladder cancer.
Evidence acquisition: Published and unpublished trials were sought via searches of bibliographic databases, trials registers, conference proceedings, and hand searching. Updated IPD were centrally collected, checked, and analysed. Results from individual randomised controlled trials (RCTs) were combined using a two-stage fixed-effect model. Prespecified analyses explored any variation in effect by trial and participant characteristics.
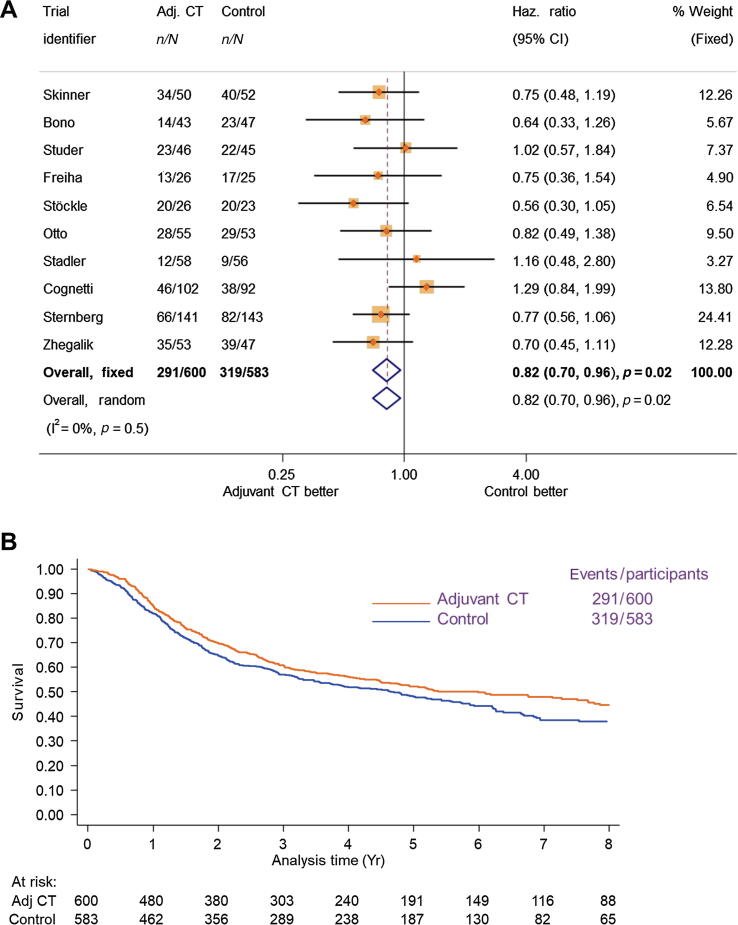
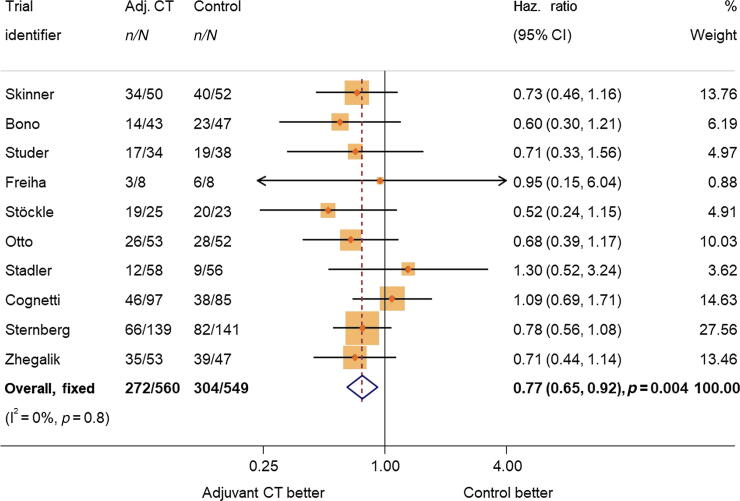
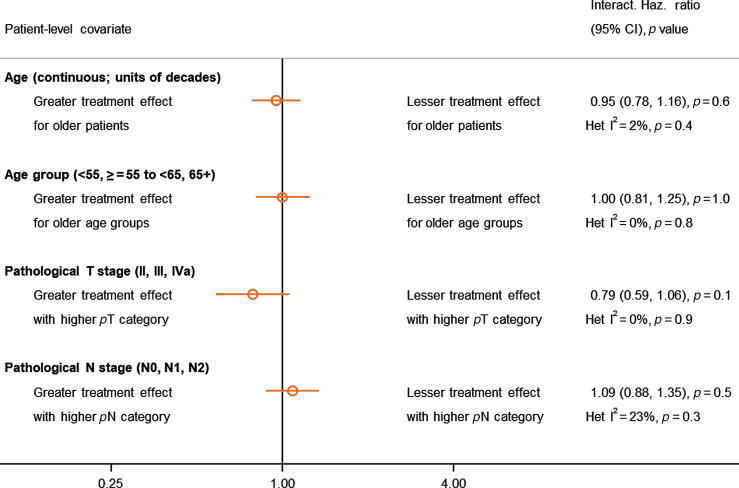
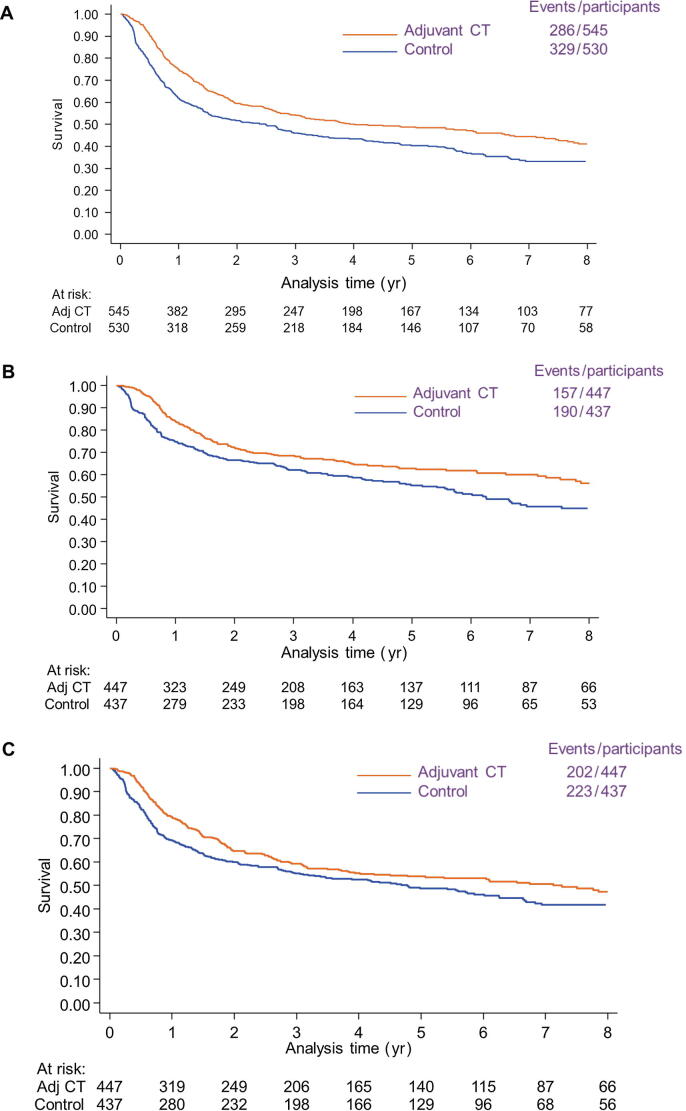
Evidence synthesis: Analyses of ten RCTs (1183 participants) demonstrated a benefit of cisplatin-based adjuvant chemotherapy on overall survival (hazard ratio [HR] = 0.82, 95% confidence interval [CI] = 0.70-0.96, p = 0.02). This represents an absolute improvement in survival of 6% at 5 yr, from 50% to 56%, and a 9% absolute benefit when adjusted for age, sex, pT stage, and pN category (HR = 0.77, 95% CI = 0.65-0.92, p = 0.004). There was no clear evidence that the effect varied by trial or participant characteristics. Adjuvant chemotherapy was also shown to improve recurrence-free survival (HR = 0.71, 95% CI = 0.60-0.83, p < 0.001), locoregional recurrence-free survival (HR = 0.68, 95% CI = 0.55-0.85, p < 0.001), and metastasis-free survival (HR = 0.79, 95% CI = 0.65-0.95, p = 0.01), with absolute benefits of 11%, 11%, and 8%, respectively.
Conclusions: This systematic review and meta-analysis demonstrates that cisplatin-based adjuvant chemotherapy is a valid option for improving outcomes for muscle-invasive bladder cancer.
Patient summary: We looked at the effect of cisplatin-based chemotherapy on outcomes in participants with muscle-invasive bladder cancer. We gathered this information from eligible randomised controlled trials. We demonstrated that cisplatin-based chemotherapy is a valid option for improving outcomes of muscle-invasive bladder cancer.
Keywords: Bladder cancer; Chemotherapy; Individual participant data; Meta-analysis; Systematic review.
Copyright © 2021 The Authors. Published by Elsevier B.V. All rights reserved.
Figures
Comment in
-
Placing Adjuvant Chemotherapy in the Evolving Paradigm of Perioperative Therapy for Bladder Cancer.Eur Urol. 2022 Jan;81(1):62-63. doi: 10.1016/j.eururo.2021.10.020. Epub 2021 Nov 5. Eur Urol. 2022. PMID: 34750037 No abstract available.
References
-
- Advanced Bladder Cancer (ABC) Meta-analysis Collaboration Adjuvant chemotherapy in invasive bladder cancer: a systematic review and meta-analysis of individual patient data. Eur Urol. 2005;48:189–201. - PubMed
-
- Paz-Ares L., Solsona E., Esteban E., et al. Randomized phase III trial comparing adjuvant paclitaxel/gemcitabine/cisplatin (PGC) to observation in patients with resected invasive bladder cancer: results of the SOGUG (Spanish Oncology Genito-Urinary Group) 99/01 study. J Clin Oncol. 2010;28(18 suppl):LBA4518.
-
- Cognetti F., Ruggeri E.M., Felici A., et al. Adjuvant chemotherapy with cisplatin and gemcitabine versus chemotherapy at relapse in patients with muscle-invasive bladder cancer submitted to radical cystectomy: an Italian, multicenter, randomized phase III trial. Ann Oncol. 2012;23:695–700. - PubMed
-
- Sternberg C.N., Skoneczna I., Kerst J.M., Albers P., Fossa S.D., Agerbaek M., et al. Immediate versus deferred chemotherapy after radical cystectomy in patients with pT3-pT4 or N+ M0 urothelial carcinoma of the bladder (EORTC 30994): an intergroup, open label, randomised phase 3 trial. Lancet Oncol. 2015;16:76–86. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
