

Early Stopping in Experimentation With Real-Time Functional Magnetic Resonance Imaging Using a Modified Sequential Probability Ratio Test
- PMID: 34803577
- PMCID: PMC8600259
- DOI: 10.3389/fnins.2021.643740
Early Stopping in Experimentation With Real-Time Functional Magnetic Resonance Imaging Using a Modified Sequential Probability Ratio Test
Abstract
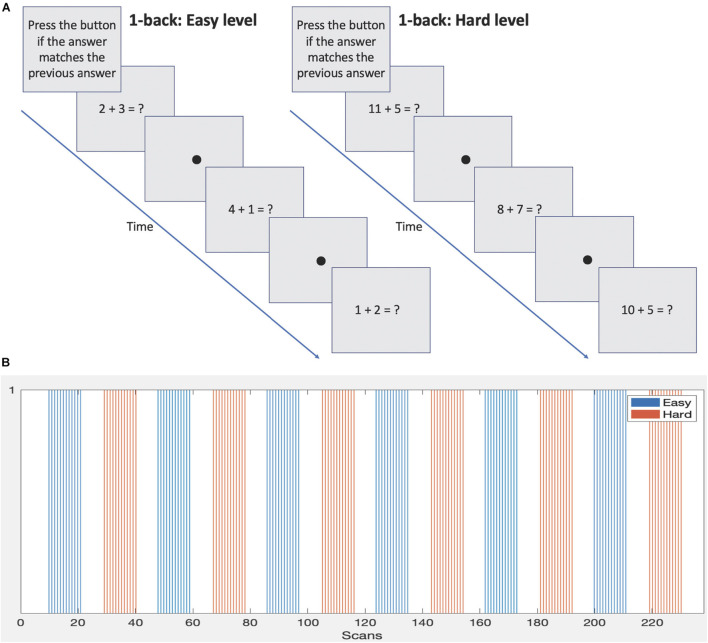
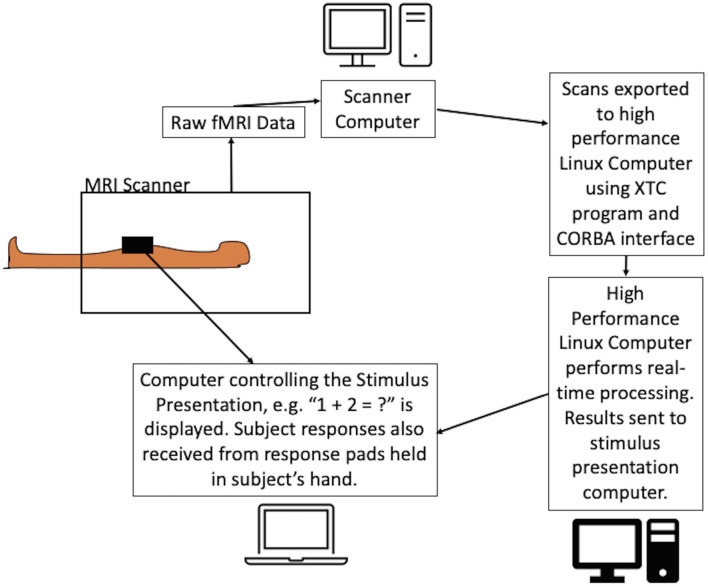
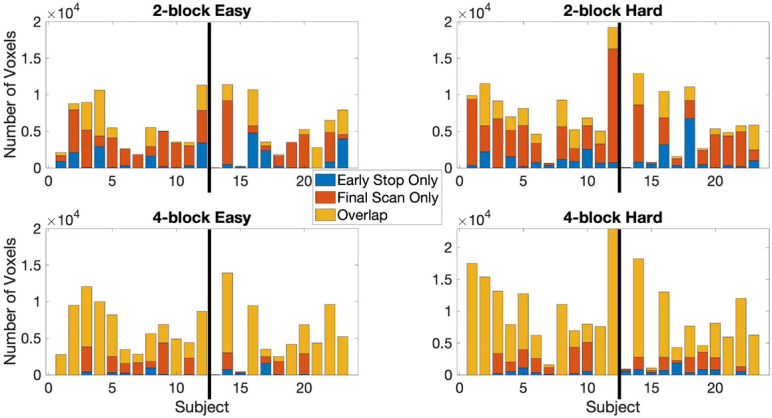
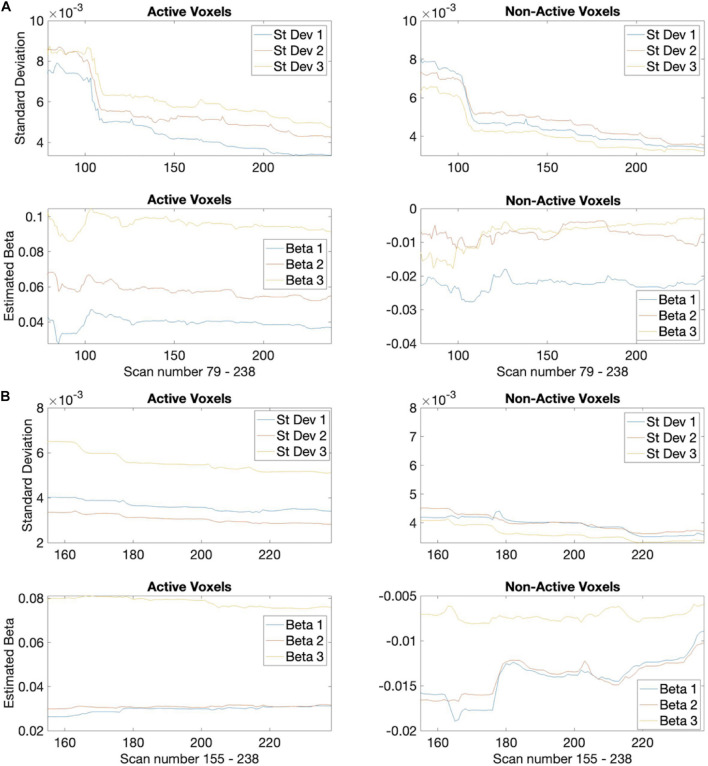
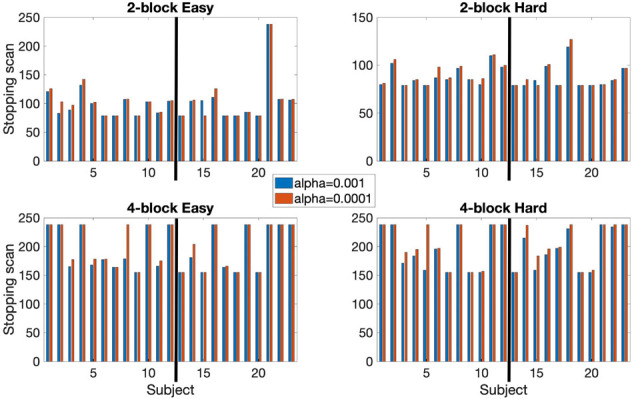
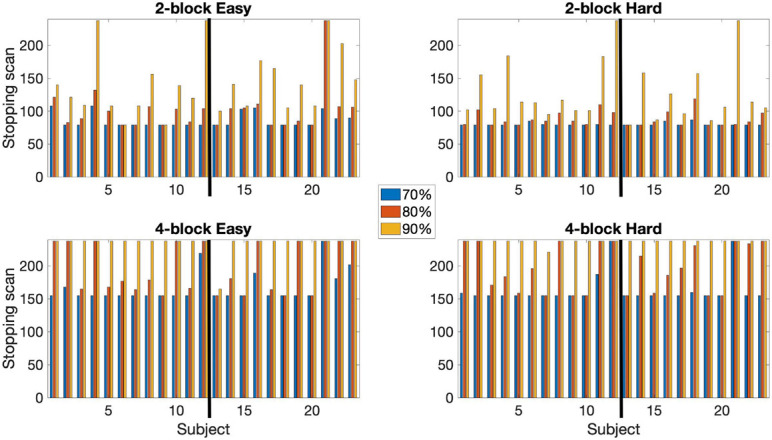
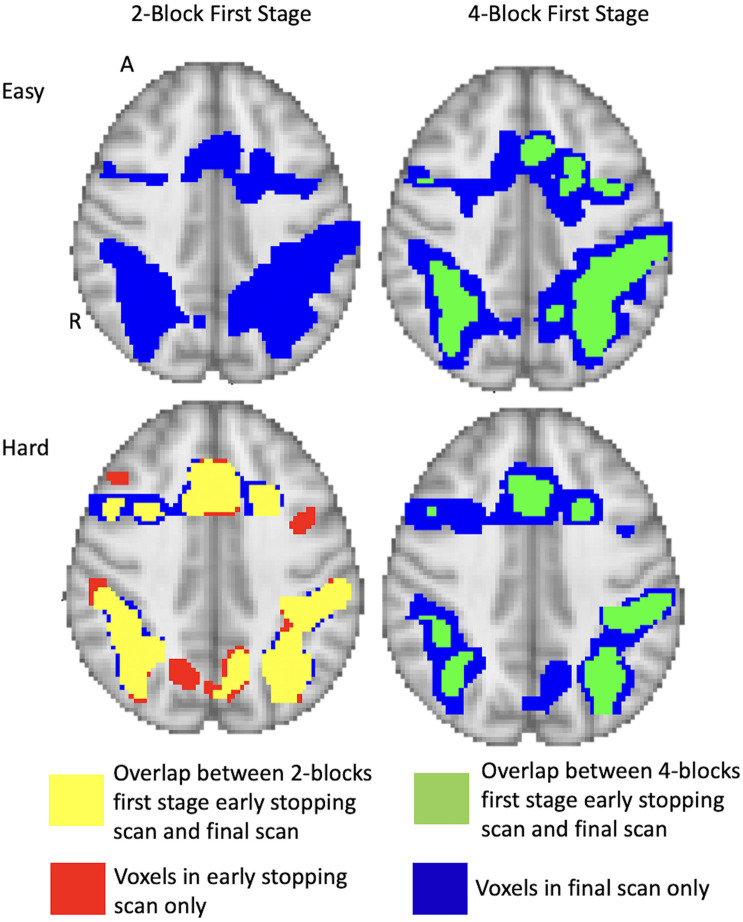
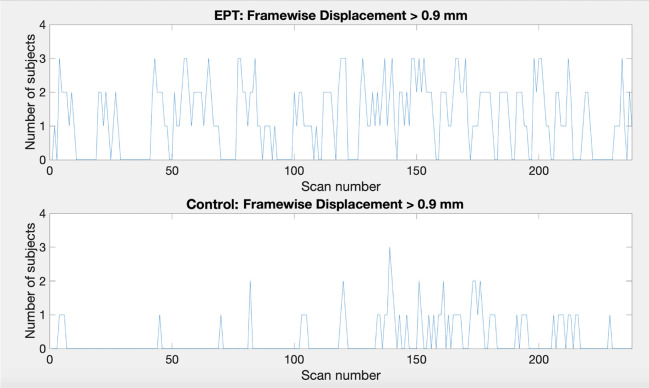
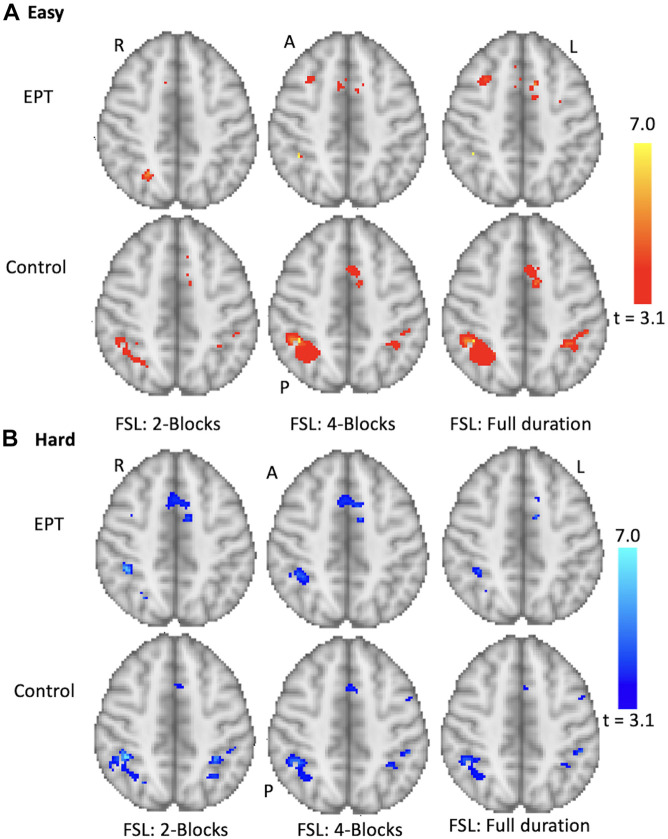
Introduction: Functional magnetic resonance imaging (fMRI) often involves long scanning durations to ensure the associated brain activity can be detected. However, excessive experimentation can lead to many undesirable effects, such as from learning and/or fatigue effects, discomfort for the subject, excessive motion artifacts and loss of sustained attention on task. Overly long experimentation can thus have a detrimental effect on signal quality and accurate voxel activation detection. Here, we propose dynamic experimentation with real-time fMRI using a novel statistically driven approach that invokes early stopping when sufficient statistical evidence for assessing the task-related activation is observed. Methods: Voxel-level sequential probability ratio test (SPRT) statistics based on general linear models (GLMs) were implemented on fMRI scans of a mathematical 1-back task from 12 healthy teenage subjects and 11 teenage subjects born extremely preterm (EPT). This approach is based on likelihood ratios and allows for systematic early stopping based on target statistical error thresholds. We adopt a two-stage estimation approach that allows for accurate estimates of GLM parameters before stopping is considered. Early stopping performance is reported for different first stage lengths, and activation results are compared with full durations. Finally, group comparisons are conducted with both early stopped and full duration scan data. Numerical parallelization was employed to facilitate completion of computations involving a new scan within every repetition time (TR). Results: Use of SPRT demonstrates the feasibility and efficiency gains of automated early stopping, with comparable activation detection as with full protocols. Dynamic stopping of stimulus administration was achieved in around half of subjects, with typical time savings of up to 33% (4 min on a 12 min scan). A group analysis produced similar patterns of activity for control subjects between early stopping and full duration scans. The EPT group, individually, demonstrated more variability in location and extent of the activations compared to the normal term control group. This was apparent in the EPT group results, reflected by fewer and smaller clusters. Conclusion: A systematic statistical approach for early stopping with real-time fMRI experimentation has been implemented. This dynamic approach has promise for reducing subject burden and fatigue effects.
Keywords: SPRT (sequential probability ratio test); adaptive fMRI; dynamic experimentation; early stopping fMRI; real-time fMRI.
Copyright © 2021 Carr, Chen, Fondran, Friel, Sanchez-Gonzalez, Zhang and Tatsuoka.
Conflict of interest statement
HF was employed by the company Philips Healthcare, USA. JS-G was employed by the company Philips Healthcare, Spain. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The authors declare that this study received funding from Philips Healthcare. The funder had the following involvement in the study: technical support and software development for the real-time output of fMRI files and revision of the manuscript.
Figures
References
-
- Carroll R. J., Wang S., Simpson D. G., Stromberg A. J., Ruppert D. (1998). The Sandwich (Robust Covariance Matrix) Estimator. Texas: Texas A&M University.
Grants and funding
LinkOut - more resources
Full Text Sources