

Perspective on Vision Science-Informed Interventions for Central Vision Loss
- PMID: 34803584
- PMCID: PMC8599964
- DOI: 10.3389/fnins.2021.734970
Perspective on Vision Science-Informed Interventions for Central Vision Loss
Abstract
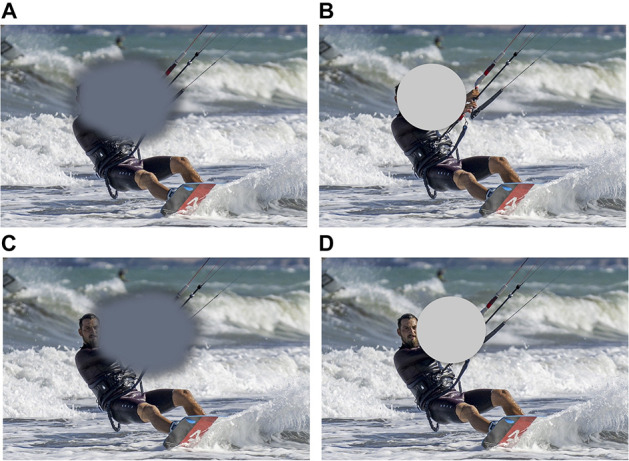
Pathologies affecting central vision, and macular degeneration (MD) in particular, represent a growing health concern worldwide, and the leading cause of blindness in the Western World. To cope with the loss of central vision, MD patients often develop compensatory strategies, such as the adoption of a Preferred Retinal Locus (PRL), which they use as a substitute fovea. However, visual acuity and fixation stability in the visual periphery are poorer, leaving many MD patients struggling with tasks such as reading and recognizing faces. Current non-invasive rehabilitative interventions are usually of two types: oculomotor, aiming at training eye movements or teaching patients to use or develop a PRL, or perceptual, with the goal of improving visual abilities in the PRL. These training protocols are usually tested over a series of outcome assessments mainly measuring low-level visual abilities (visual acuity, contrast sensitivity) and reading. However, extant approaches lead to mixed success, and in general have exhibited large individual differences. Recent breakthroughs in vision science have shown that loss of central vision affects not only low-level visual abilities and oculomotor mechanisms, but also higher-level attentional and cognitive processes. We suggest that effective interventions for rehabilitation after central vision loss should then not only integrate low-level vision and oculomotor training, but also take into account higher level attentional and cognitive mechanisms.
Keywords: clinical intervention strategy perspective; macular degeneration; neural plasticity; oculomotor abilities; perceptual learning; visual rehabilitation.
Copyright © 2021 Maniglia, Visscher and Seitz.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



Similar articles
-
Consistency of preferred retinal locus across tasks and participants trained with a simulated scotoma.Vision Res. 2023 Feb;203:108158. doi: 10.1016/j.visres.2022.108158. Epub 2022 Dec 15. Vision Res. 2023. PMID: 36527839 Free PMC article.
-
A Gaze-Contingent Display Framework for Perceptual Learning Research with Simulated Central Vision Loss.J Vis Exp. 2025 Apr 11;(218). doi: 10.3791/67596. J Vis Exp. 2025. PMID: 40293961
-
Combining fixation and lateral masking training enhances perceptual learning effects in patients with macular degeneration.J Vis. 2020 Oct 1;20(10):19. doi: 10.1167/jov.20.10.19. J Vis. 2020. PMID: 33064123 Free PMC article.
-
Neural and perceptual adaptations in bilateral macular degeneration: an integrative review.Neuropsychologia. 2025 Aug 13;215:109165. doi: 10.1016/j.neuropsychologia.2025.109165. Epub 2025 May 8. Neuropsychologia. 2025. PMID: 40345486 Review.
-
Binocular visual function and fixational control in patients with macular disease: A review.Ophthalmic Physiol Opt. 2022 Mar;42(2):258-271. doi: 10.1111/opo.12925. Epub 2021 Dec 4. Ophthalmic Physiol Opt. 2022. PMID: 34862635 Free PMC article. Review.
Cited by
-
Current directions in visual perceptual learning.Nat Rev Psychol. 2022 Nov;1(11):654-668. doi: 10.1038/s44159-022-00107-2. Epub 2022 Sep 27. Nat Rev Psychol. 2022. PMID: 37274562 Free PMC article.
-
Enabling identification of component processes in perceptual learning with nonparametric hierarchical Bayesian modeling.J Vis. 2024 May 1;24(5):8. doi: 10.1167/jov.24.5.8. J Vis. 2024. PMID: 38780934 Free PMC article.
-
Hierarchical Bayesian Augmented Hebbian Reweighting Model of Perceptual Learning.bioRxiv [Preprint]. 2024 Aug 9:2024.08.08.606902. doi: 10.1101/2024.08.08.606902. bioRxiv. 2024. Update in: J Vis. 2025 Apr 1;25(4):9. doi: 10.1167/jov.25.4.9. PMID: 39149245 Free PMC article. Updated. Preprint.
-
Topical Review: Impact of Central Vision Loss on Navigation and Obstacle Avoidance while Walking.Optom Vis Sci. 2022 Dec 1;99(12):890-899. doi: 10.1097/OPX.0000000000001960. Epub 2022 Nov 26. Optom Vis Sci. 2022. PMID: 36594757 Free PMC article.
-
The effect of duration between sessions on microperimetric biofeedback training in patients with maculopathies.Sci Rep. 2024 May 31;14(1):12524. doi: 10.1038/s41598-024-63327-x. Sci Rep. 2024. PMID: 38822030 Free PMC article.