

The Effect of a Combined Ganciclovir, Methylprednisolone, and Immunoglobulin Regimen on Survival and Functional Outcomes in Patients With Japanese Encephalitis
- PMID: 34803868
- PMCID: PMC8600080
- DOI: 10.3389/fneur.2021.711674
The Effect of a Combined Ganciclovir, Methylprednisolone, and Immunoglobulin Regimen on Survival and Functional Outcomes in Patients With Japanese Encephalitis
Abstract
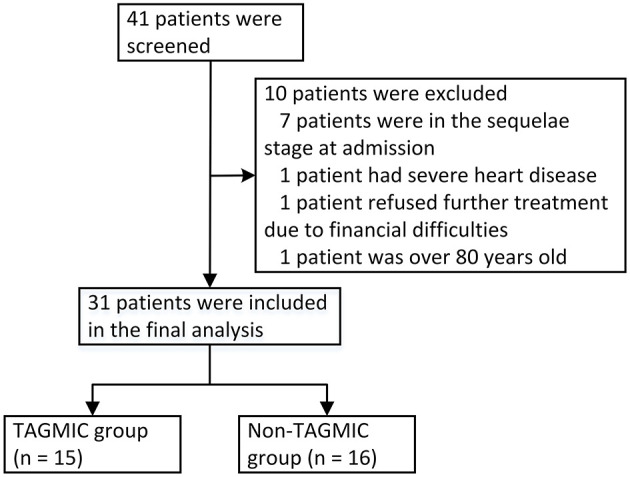
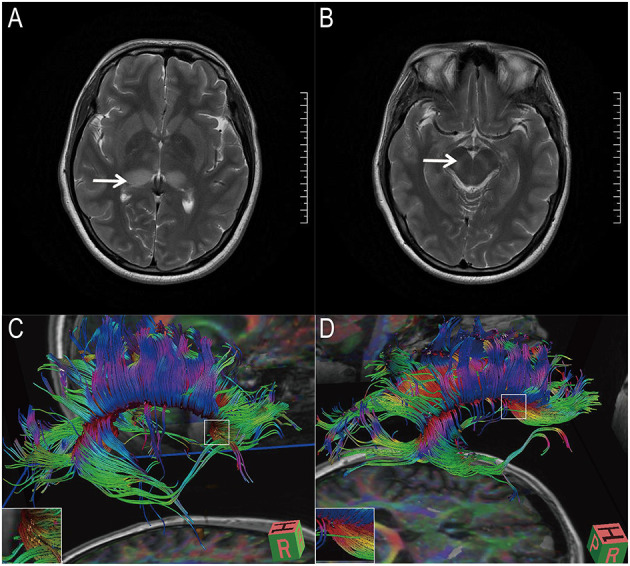
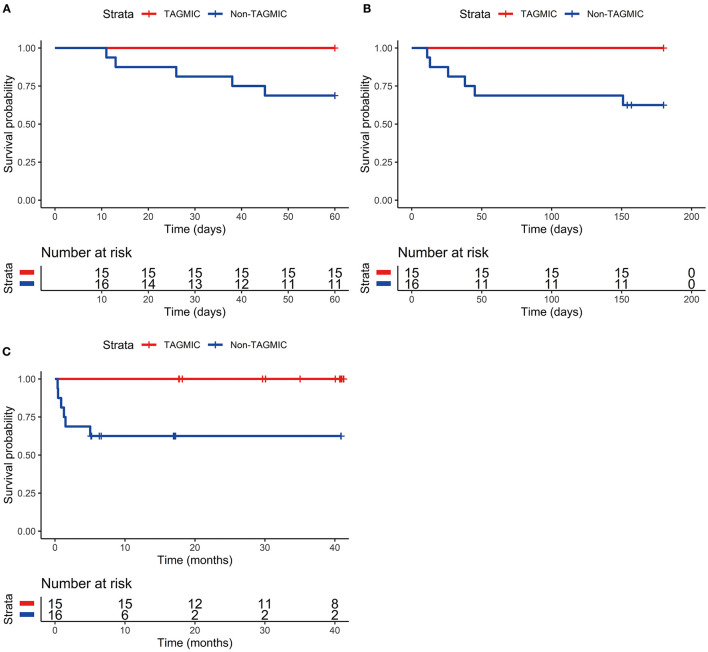
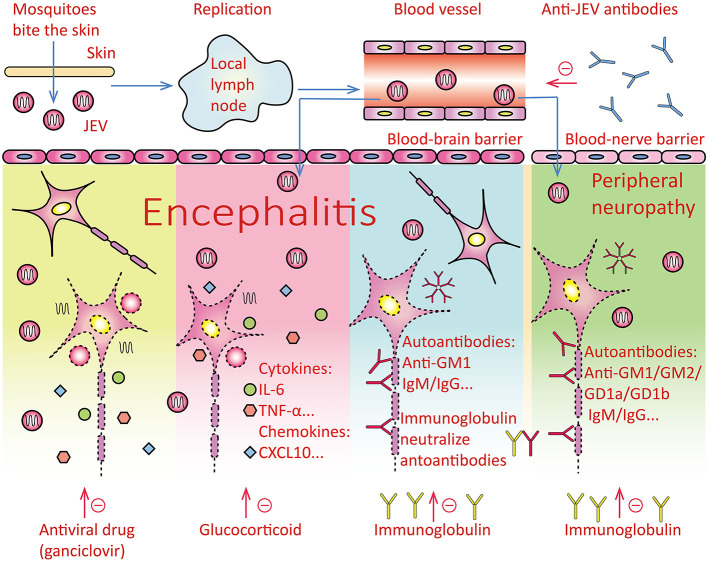
Objective: There is currently no effective treatment for Japanese encephalitis, which has a high rate of morbidity and mortality. This study assessed the effectiveness of a ganciclovir, methylprednisolone, and immunoglobulin combination (TAGMIC) therapy in decreasing cognitive impairment and mortality among patients with Japanese encephalitis. Methods: We retrospectively assessed the clinical data of 31 patients diagnosed with Japanese encephalitis, who were admitted to an intensive care unit. Patients were divided into the TAGMIC and non-TAGMIC group according to their treatment regime. We compared the 60-day, 6-month, and overall mortality and survival curves between groups. We also compared Barthel Index scores, Montreal Cognitive Assessment (MoCA) scores, and diffusion tensor imaging (DTI) results. Results: There was no significant difference in the 30-day mortality rate or Kaplan-Meier survival curve between groups. The 60-day, 6-month, and overall mortality rates in the TAGMIC group were significantly reduced (P = 0.043, P = 0.018, and P = 0.018, respectively) compared with the non-TAGMIC group (0, 0, 0 vs. 31.25, 37.5, 37.5%, respectively). The 60-day, 6-month, and overall Kaplan-Meier survival curves were significantly different between groups (P = 0.020, P = 0.009, P = 0.009, respectively). There was no significant difference in the Barthel Index scores of surviving patients. Among the five patients who underwent MoCA and DTI, four had a score of 0/5 for delayed recall (no cue), while the remaining patient had a score of 2/5. All five patients were able to achieve a score of 5/5 with classification and multiple-choice prompts, and had sparse or broken corpus callosum (or other) fibre bundles. Conclusion: TAGMIC treatment can reduce mortality due to severe Japanese encephalitis. The memory loss of surviving patients is mainly due to a disorder of the memory retrieval process, which may be related to the breakage of related fibre bundles.
Keywords: Japanese encephalitis; combined regimen; ganciclovir; immunoglobulin; methylprednisolone.
Copyright © 2021 Miao, Guo, Zhang, Shen, Shang, Liu, Lu, Xu and Teng.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Clinical Characteristics of Cognitive Impairment and 1-Year Outcome in Patients With Anti-LGI1 Antibody Encephalitis.Front Neurol. 2020 Aug 21;11:852. doi: 10.3389/fneur.2020.00852. eCollection 2020. Front Neurol. 2020. PMID: 33162923 Free PMC article.
-
[Effects of early intervention training on cognitive impairment in critical patients].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2019 Mar;31(3):298-302. doi: 10.3760/cma.j.issn.2095-4352.2019.03.008. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2019. PMID: 30914089 Clinical Trial. Chinese.
-
[Value of procalcitonin on predicting the severity and prognosis in patients with early ARDS: a prospective observation study].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2017 Jan;29(1):34-38. doi: 10.3760/cma.j.issn.2095-4352.2017.01.008. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2017. PMID: 28459401 Chinese.
-
Mitoxantrone: a review of its use in multiple sclerosis.CNS Drugs. 2004;18(6):379-96. doi: 10.2165/00023210-200418060-00010. CNS Drugs. 2004. PMID: 15089110 Review.
-
Retrospective case analysis of antiviral therapies for HHV-6 encephalitis after hematopoietic stem cell transplantation.Transpl Infect Dis. 2021 Feb;23(1):e13443. doi: 10.1111/tid.13443. Epub 2020 Sep 1. Transpl Infect Dis. 2021. PMID: 32786154 Review.
Cited by
-
Treatment of Severe Japanese Encephalitis Complicated With Hashimoto's Thyroiditis and Guillain-Barré Syndrome With Protein A Immunoadsorption: A Case Report.Front Immunol. 2022 Jan 7;12:807937. doi: 10.3389/fimmu.2021.807937. eCollection 2021. Front Immunol. 2022. PMID: 35069593 Free PMC article.
-
Clinical characteristics and short-term outcomes of Japanese encephalitis in pediatric and adult patients: a retrospective study in Northern China.Front Neurol. 2023 Apr 20;14:1135001. doi: 10.3389/fneur.2023.1135001. eCollection 2023. Front Neurol. 2023. PMID: 37153674 Free PMC article.
-
Human parvovirus B19 infection in hospitalized patients suspected of infection with pathogenic microorganism.Front Cell Infect Microbiol. 2022 Dec 21;12:1083839. doi: 10.3389/fcimb.2022.1083839. eCollection 2022. Front Cell Infect Microbiol. 2022. PMID: 36619750 Free PMC article.
References
-
- WHO . Japanese Encephalitis. (2019). Available online at: https://www.who.int/news-room/fact-sheets/detail/japanese-encephalitis.
LinkOut - more resources
Full Text Sources