

The Onset of Interictal Spike-Related Ripples Facilitates Detection of the Epileptogenic Zone
- PMID: 34803874
- PMCID: PMC8599368
- DOI: 10.3389/fneur.2021.724417
The Onset of Interictal Spike-Related Ripples Facilitates Detection of the Epileptogenic Zone
Abstract
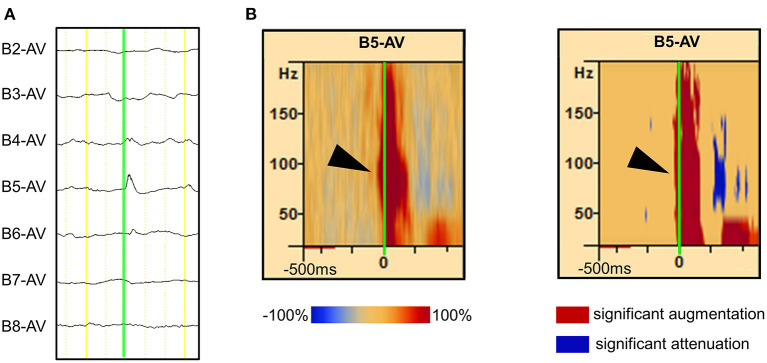
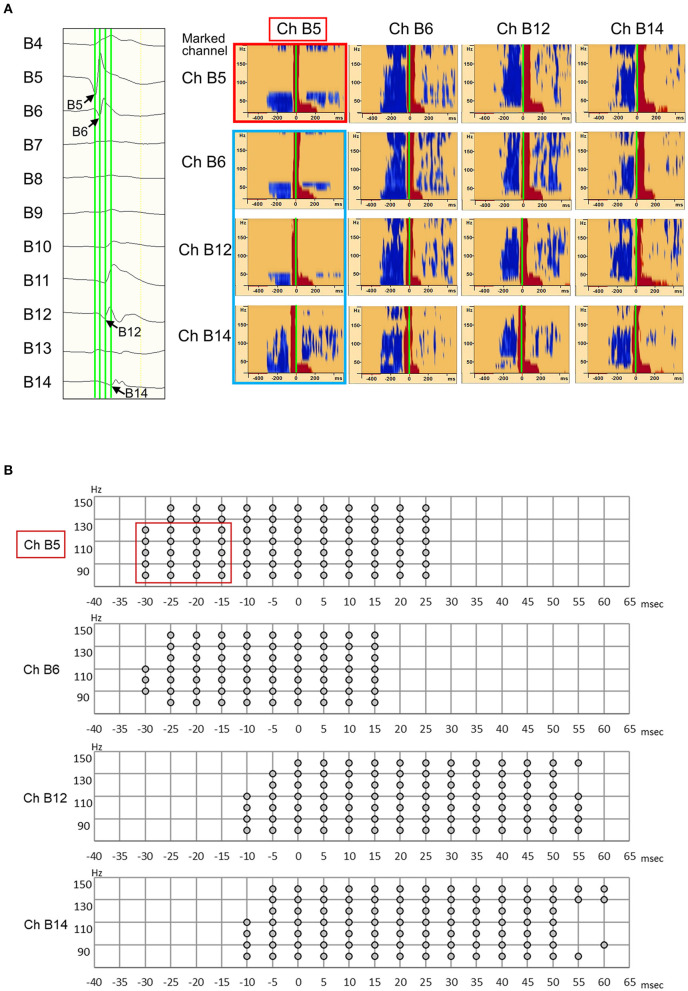
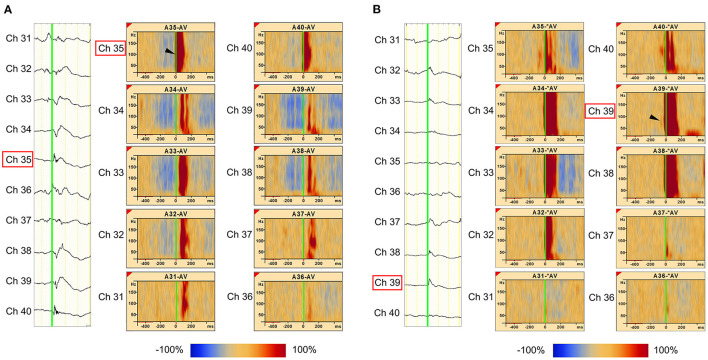
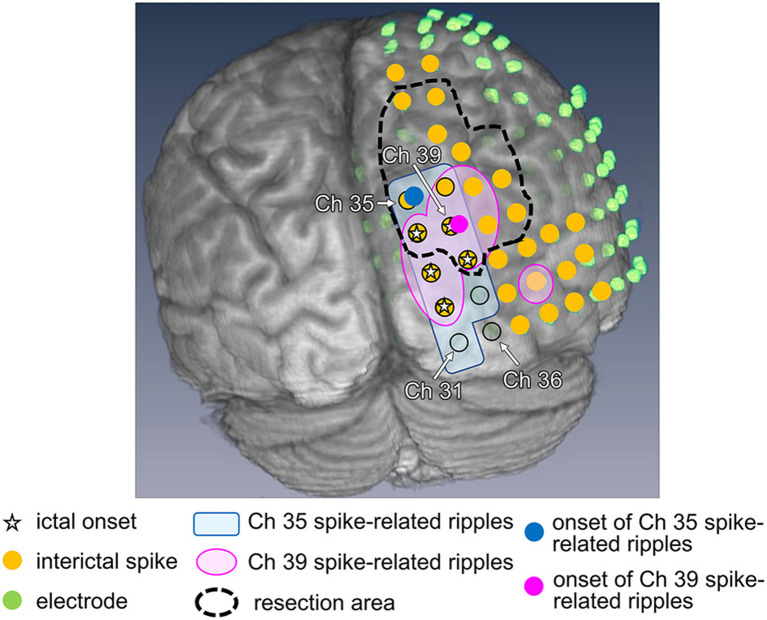
Objective: Accurate estimation of the epileptogenic zone (EZ) is essential for favorable outcomes in epilepsy surgery. Conventional ictal electrocorticography (ECoG) onset is generally used to detect the EZ but is insufficient in achieving seizure-free outcomes. By contrast, high-frequency oscillations (HFOs) could be useful markers of the EZ. Hence, we aimed to detect the EZ using interictal spikes and investigated whether the onset area of interictal spike-related HFOs was within the EZ. Methods: The EZ is considered to be included in the resection area among patients with seizure-free outcomes after surgery. Using a complex demodulation technique, we developed a method to determine the onset channels of interictal spike-related ripples (HFOs of 80-200 Hz) and investigated whether they are within the resection area. Results: We retrospectively examined 12 serial patients who achieved seizure-free status after focal resection surgery. Using the method that we developed, we determined the onset channels of interictal spike-related ripples and found that for all 12 patients, they were among the resection channels. The onset frequencies of ripples were in the range of 80-150 Hz. However, the ictal onset channels (evaluated based on ictal ECoG patterns) and ripple onset channels coincided in only 3 of 12 patients. Conclusions: Determining the onset area of interictal spike-related ripples could facilitate EZ estimation. This simple method that utilizes interictal ECoG may aid in preoperative evaluation and improve epilepsy surgery outcomes.
Keywords: epilepsy; epileptogenic zone; interictal; onset; spike-related ripples; surgery.
Copyright © 2021 Numata-Uematsu, Uematsu, Sakuraba, Iwasaki, Osawa, Jin, Nakasato and Kure.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources