

Selective Inhibitor of the c-Met Receptor Tyrosine Kinase in Advanced Hepatocellular Carcinoma: No Beneficial Effect With the Use of Tivantinib?
- PMID: 34804015
- PMCID: PMC8600564
- DOI: 10.3389/fimmu.2021.731527
Selective Inhibitor of the c-Met Receptor Tyrosine Kinase in Advanced Hepatocellular Carcinoma: No Beneficial Effect With the Use of Tivantinib?
Abstract
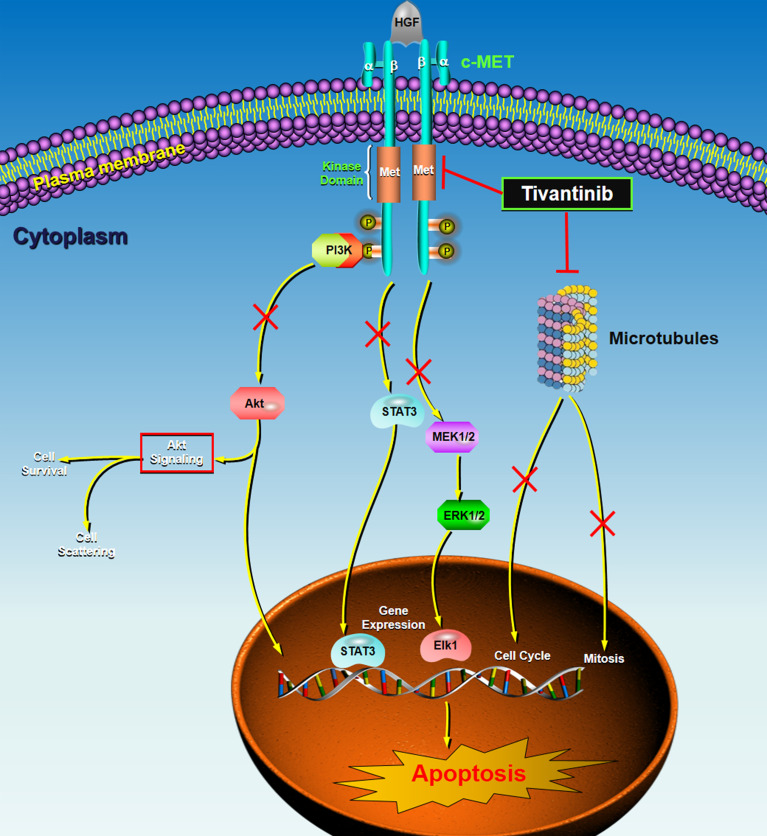
Advanced hepatocellular carcinoma (HCC) remains a formidable health challenge worldwide, with a 5-year survival rate of 2.4% in patients with distant metastases. The hepatocyte growth factor/cellular-mesenchymal-epithelial transition (HGF/c-Met) signaling pathway represents an encouraging therapeutic target for progressive HCC. Tivantinib, a non-adenosine triphosphate-competitive c-Met inhibitor, showed an attractive therapeutic effect on advanced HCC patients with high MET-expression in phase 2 study but failed to meet its primary endpoint of prolonging the overall survival (OS) in two phase 3 HCC clinical trials. Seven clinical trials have been registered in the "ClinicalTrials.gov" for investigating the safety and efficacy of tivantinib in treating advanced or unresectable HCC. Eight relevant studies have been published with results. The sample size ranged from 20 to 340 patients. The methods of tivantinib administration and dosage were orally 120/240/360 mg twice daily. MET overexpression was recorded at 34.6% to 100%. Two large sample phase 3 studies (the METIV-HCC study of Australia and European population and the JET-HCC study of the Japanese population) revealed that tivantinib failed to show survival benefits in advanced HCC. Common adverse events with tivantinib treatment include neutropenia, ascites, rash, and anemia, etc. Several factors may contribute to the inconsistency between the phase 2 and phase 3 studies of tivantinib, including the sample size, drug dosing, study design, and the rate of MET-High. In the future, high selective MET inhibitors combined with a biomarker-driven patient selection may provide a potentially viable therapeutic strategy for patients with advanced HCC.
Keywords: MET inhibitor; adverse event; hepatocellular carcinoma; therapeutic effect; tivantinib.
Copyright © 2021 Zhao, Wu, Jiang, Ma, Pan, Jin, Mo, Wang and Wang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Tivantinib for second-line treatment of MET-high, advanced hepatocellular carcinoma (METIV-HCC): a final analysis of a phase 3, randomised, placebo-controlled study.Lancet Oncol. 2018 May;19(5):682-693. doi: 10.1016/S1470-2045(18)30146-3. Epub 2018 Apr 3. Lancet Oncol. 2018. PMID: 29625879 Clinical Trial.
-
Tivantinib: critical review with a focus on hepatocellular carcinoma.Expert Opin Investig Drugs. 2014 Nov;23(11):1563-74. doi: 10.1517/13543784.2014.949339. Expert Opin Investig Drugs. 2014. PMID: 25307444 Review.
-
Tivantinib for second-line treatment of advanced hepatocellular carcinoma: a randomised, placebo-controlled phase 2 study.Lancet Oncol. 2013 Jan;14(1):55-63. doi: 10.1016/S1470-2045(12)70490-4. Epub 2012 Nov 20. Lancet Oncol. 2013. PMID: 23182627 Clinical Trial.
-
Tivantinib in hepatocellular carcinoma.Expert Opin Investig Drugs. 2013 Jan;22(1):141-7. doi: 10.1517/13543784.2013.741586. Epub 2012 Nov 21. Expert Opin Investig Drugs. 2013. PMID: 23167786 Review.
-
Phase I study of tivantinib in Japanese patients with advanced hepatocellular carcinoma: Distinctive pharmacokinetic profiles from other solid tumors.Cancer Sci. 2015 May;106(5):611-7. doi: 10.1111/cas.12644. Epub 2015 Apr 7. Cancer Sci. 2015. PMID: 25711511 Free PMC article. Clinical Trial.
Cited by
-
Hepatocellular carcinoma: signaling pathways and therapeutic advances.Signal Transduct Target Ther. 2025 Feb 7;10(1):35. doi: 10.1038/s41392-024-02075-w. Signal Transduct Target Ther. 2025. PMID: 39915447 Free PMC article. Review.
-
Translocations and Gene Fusions in Sinonasal Malignancies.Curr Oncol Rep. 2023 Apr;25(4):269-278. doi: 10.1007/s11912-023-01364-x. Epub 2023 Feb 8. Curr Oncol Rep. 2023. PMID: 36753024 Free PMC article. Review.
-
New and Old Key Players in Liver Cancer.Int J Mol Sci. 2023 Dec 5;24(24):17152. doi: 10.3390/ijms242417152. Int J Mol Sci. 2023. PMID: 38138981 Free PMC article. Review.
-
Recent advances in the treatment of non-small cell lung cancer with MET inhibitors.Front Chem. 2024 Dec 10;12:1501844. doi: 10.3389/fchem.2024.1501844. eCollection 2024. Front Chem. 2024. PMID: 39720556 Free PMC article. Review.
-
Tumor biomarkers for diagnosis, prognosis and targeted therapy.Signal Transduct Target Ther. 2024 May 20;9(1):132. doi: 10.1038/s41392-024-01823-2. Signal Transduct Target Ther. 2024. PMID: 38763973 Free PMC article. Review.
References
-
- Vogel A, Qin S, Kudo M, Su Y, Hudgens S, Yamashita T, et al. . Lenvatinib Versus Sorafenib for First-Line Treatment of Unresectable Hepatocellular Carcinoma: Patient-Reported Outcomes From a Randomised, Open-Label, non-Inferiority, Phase 3 Trial. Lancet Gastroenterol Hepatol (2021) 6(8):649–58. doi: 10.1016/S2468-1253(21)00110-2 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous