

Effect of Intubation Timing on the Outcome of Patients With Severe Respiratory Distress Secondary to COVID-19 Pneumonia
- PMID: 34804753
- PMCID: PMC8597669
- DOI: 10.7759/cureus.19620
Effect of Intubation Timing on the Outcome of Patients With Severe Respiratory Distress Secondary to COVID-19 Pneumonia
Abstract
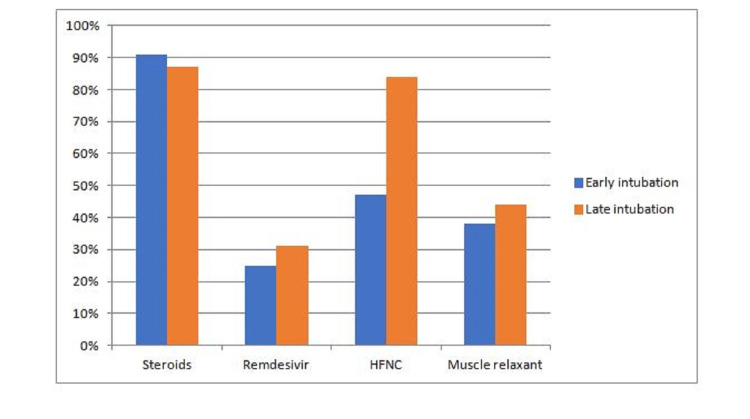
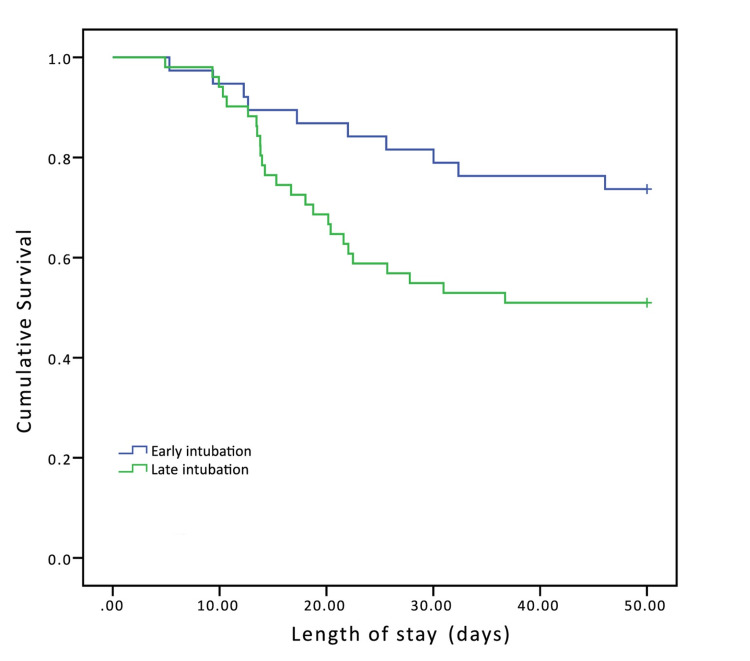
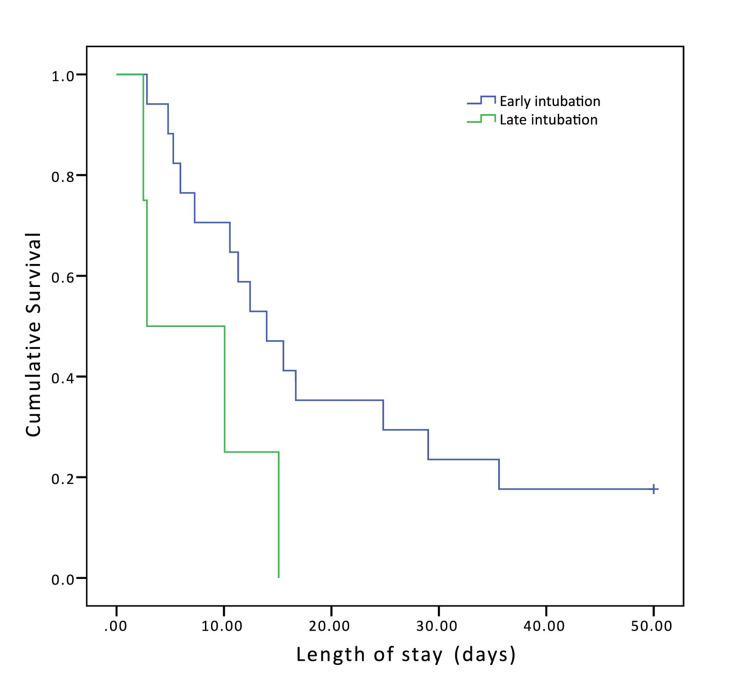
Background The optimal timing of intubation for critically ill patients with severe respiratory illness remains controversial among healthcare providers. The coronavirus disease 2019 (COVID-19) pandemic has raised even more questions about when to implement this life-saving therapy. While one group of providers prefers early intubation for patients with respiratory distress because these patients may deteriorate rapidly without it, other providers believe that intubation should be delayed or avoided because of its associated risks including worse outcomes. Research question Our objective was to assess whether the timing of intubation in patients with severe COVID-19 pneumonia was associated with differences in mortality or other outcomes. Study design and methods This was a single-center retrospective observational cohort study. We analyzed outcomes of patients who were intubated secondary to COVID-19 pneumonia between March 13, 2020, and December 12, 2020, at Henry Ford Hospital in Detroit, Michigan. Patients were categorized into two groups: early intubated (intubated within 24 hours of the onset of severe respiratory distress) and late intubated (intubated after 24 hours of the onset of severe respiratory distress). Demographics, comorbidities, respiratory rate oxygenation (ROX) index, sequential organ failure assessment (SOFA) score, and treatment received were compared between groups. The primary outcome was mortality. Secondary outcomes were ventilation time, intensive care unit stay, hospital length of stay, and discharge disposition. Post hoc and Kaplan-Meier survival analyses were performed. Results A total of 110 patients were included: 55 early intubated and 55 late intubated. We did not observe a significant difference in overall mortality between the early intubated (43%) and the late intubated groups (53%) (p = 0.34). There was no statistically significant difference in patients' baseline characteristics including SOFA scores (the early intubation group had a mean score of 7.5 compared to 6.7 in the late intubation group). Based on the ROX index, the early intubation group had significantly more patients with a reduced risk of intubation (45%) than the late group (27%) (p = 0.029). The early intubation group was treated with a high-flow nasal cannula at a significantly lower rate (47%) than the late intubation group (83%) (p < 0.001). Significant differences in patient baseline characteristics, treatment received, and other outcomes were not observed. Post hoc analysis adjusting for SOFA score between 0 and 9 revealed significantly higher mortality in the late intubation group (49%) than in the early intubation group (26%) (p = 0.03). Patients in the 0 to 9 SOFA group who were intubated later had 2.7 times the odds of dying during hospital admission compared to patients who were intubated early (CI, 1.09-6.67). Interpretation The timing of intubation for patients with severe COVID-19 pneumonia was not significantly associated with overall mortality or other patient outcomes. However, within the subgroup of patients with SOFA scores of 9 or lower at the time of intubation, patients intubated after 24 hours of the onset of respiratory distress had a higher risk of death than those who were intubated within 24 hours of respiratory distress. Thus, patients with COVID-19 pneumonia who are not at a high level of organ dysfunction may benefit from early mechanical ventilation.
Keywords: acute respiratory distress syndrome [ards]; airway intubation; covid-19 respiratory failure; high flow nasal canula; kaplan-meier survival curves; mechanical ventilation; resuscitation; rox index; severe respiratory failure; sofa score.
Copyright © 2021, Fayed et al.
Conflict of interest statement
There is no financial, consultant, or institutional conflict of interests for any of the authors. However, it is to be noted that the first author was a COVID-19 survivor and was in favor of early intubation during the course of his hospitalization. He was in the late intubation group though.
Figures
References
-
- WHO Director-General's remarks at the media briefing on 2019-nCoV on 11 February 2020. https://www.who.int/director-general/speeches/detail/who-director-genera... 2020
-
- Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. Wu Z, McGoogan JM. https://doi.org/10.1001/jama.2020.2648. JAMA. 2020;323:1239–1242. - PubMed
LinkOut - more resources
Full Text Sources