

Body composition in individuals with cystic fibrosis
- PMID: 34804808
- PMCID: PMC8586800
- DOI: 10.1016/j.jcte.2021.100272
Body composition in individuals with cystic fibrosis
Abstract
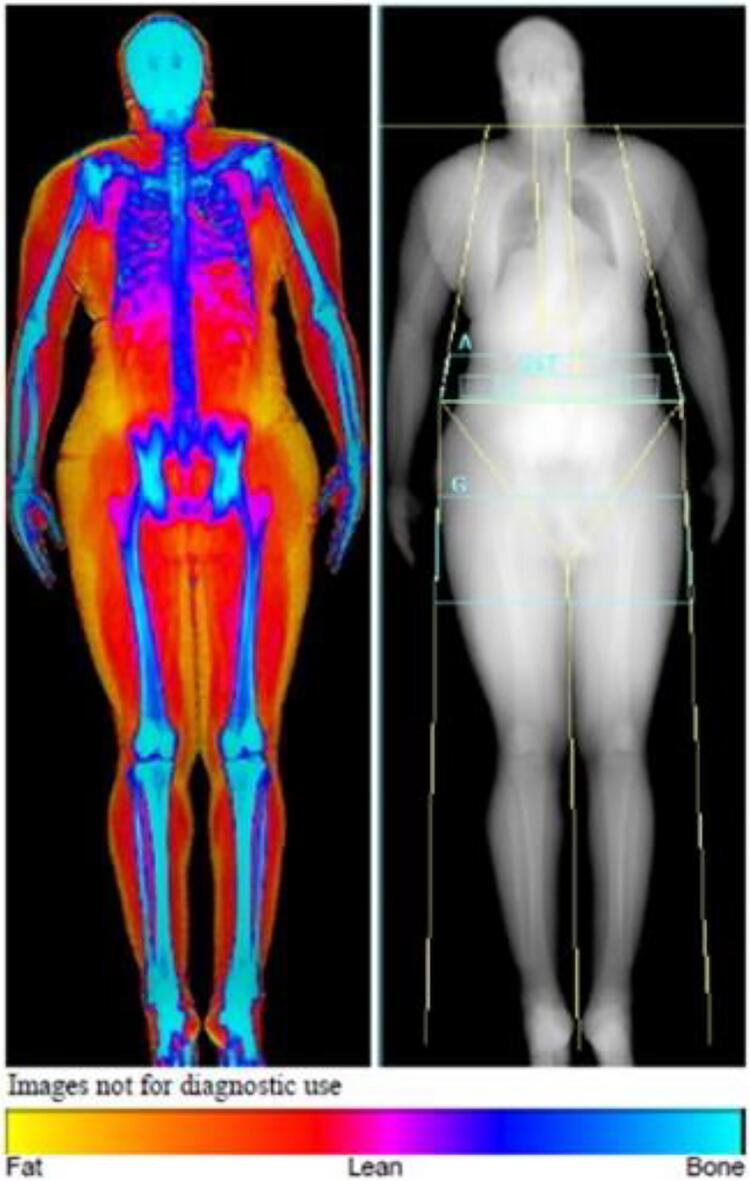
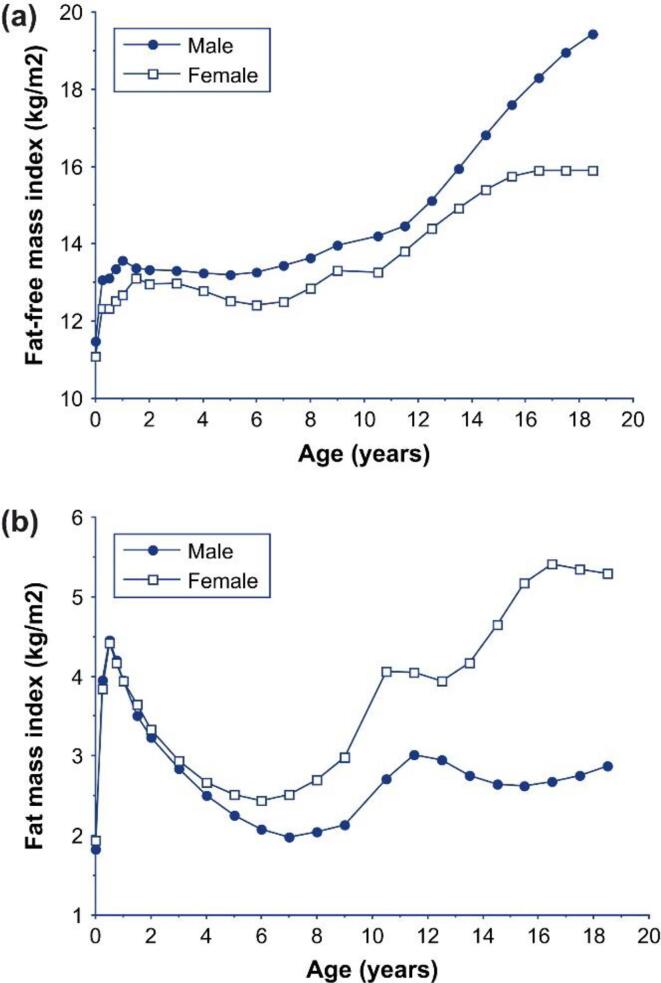
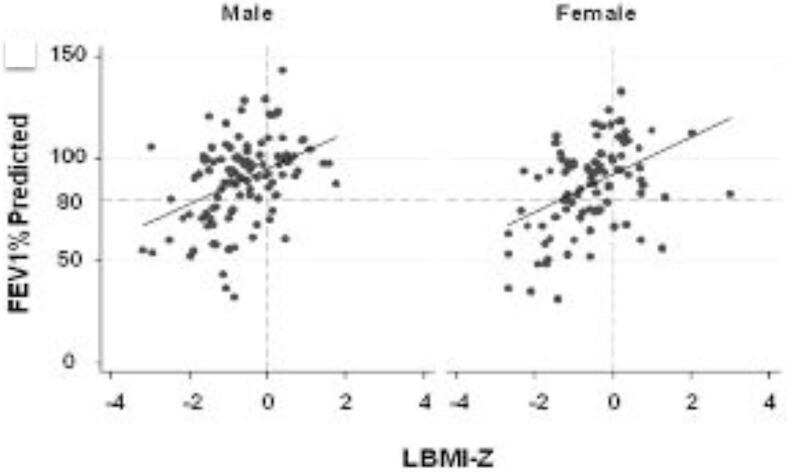
Because nutritional status is intimately linked with pulmonary function and survival, nutrition has been at the mainstay of cystic fibrosis (CF) care. Body Mass Index (BMI) is traditionally used to define nutritional status because of the ease with which it can be calculated, but it has a number of limitations including its inability to differentiate fat mass (FM) from lean body mass (LBM), the latter thought to confer health advantage. A number of tools are available to quantify body composition including dual-energy x-ray absorptiometry (DXA), bioelectrical impedance, MRI, CT, air displacement plethysmography, and stable isotopes, and these have been used to varying degrees in studies of CF. In CF, LBM tends to be lower for a given BMI, particularly at lower BMI. In adults, lower fat-free mass (FFM) correlates with greater CF disease severity, lower pulmonary function and higher inflammatory markers. FFM is also positively associated with greater bone mineral density, while greater FM is associated with greater loss of lumbar spine bone mineral density over 2 years. In youth, LBM is positively associated with pulmonary function. The predictive value of body composition for functional and clinical outcomes and the role of improving LBM on these outcomes remain undefined. With improvements in BMI accompanying highly-effective modulator therapy, closer evaluations of body composition may inform risk for more traditional, non-CF adult outcomes in CF.
Keywords: %BF, Percentage body fat; BC, Body composition; BIA, Bioelectrical impedance; BMI, Body mass index; Bioelectrical impedance; Body composition; CF, Cystic fibrosis; CFTR, Cystic fibrosis transmembrane conductance regulator; CT, Computed tomography; Cystic fibrosis; DXA, Dual-energy X-ray absorptiometry; Dual-energy X-ray absorptiometry; FFM, Fat-free mass; FFMI, Fat-free mass index; FM, Fat mass; FMI, Fat mass index; Fat mass; HEMT, Highly Effective Modulator Therapy; LBM, Lean body mass; Lean body mass; MRI, Magnetic resonance imaging.
© 2021 The Author(s).
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
LinkOut - more resources
Full Text Sources
Miscellaneous
