

Comparative outcomes of Inferior Vena Cava filters placed at bedside using digital radiography versus conventional fluoroscopy
- PMID: 34805962
- PMCID: PMC8562161
- DOI: 10.1016/j.jimed.2021.05.001
Comparative outcomes of Inferior Vena Cava filters placed at bedside using digital radiography versus conventional fluoroscopy
Abstract
Purpose: To retrospectively assess the outcomes of Inferior Vena Cava (IVC) filters placed in critically ill patients in the ICU at bedside using digital radiograph (DR) guidance with previous cross-sectional imaging for planning, compared to IVC filters placed by conventional fluoroscopy (CF).
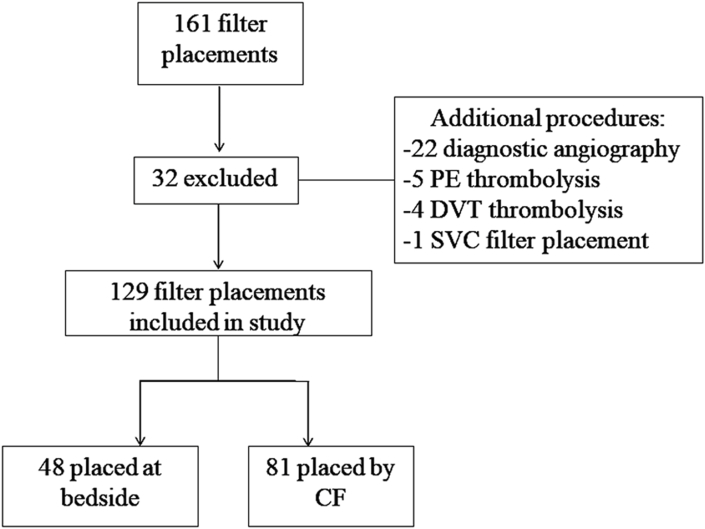
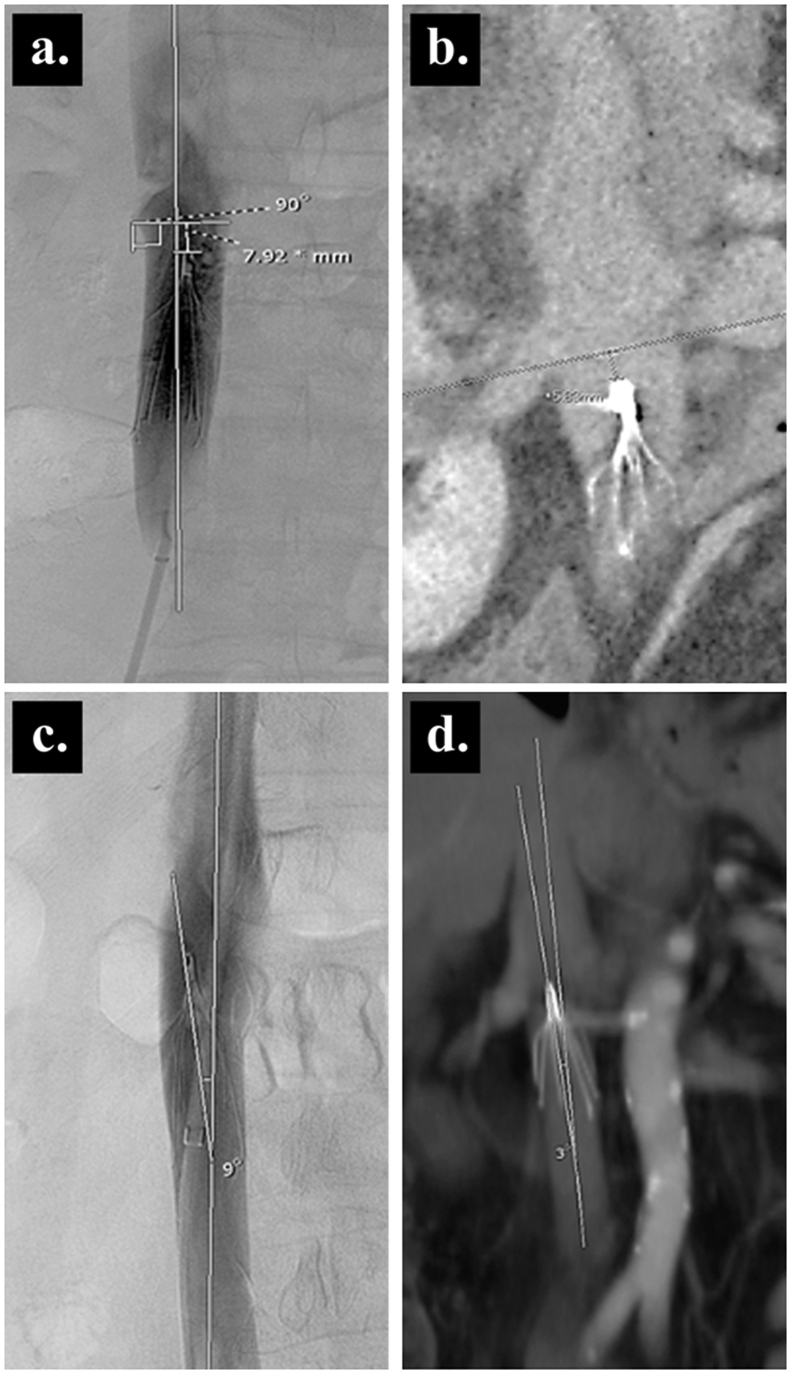
Method and materials: The cohort consisted of 129 IVC filter placements; 48 placed at bedside and 81 placed conventionally from July 2015 to September 2016. Patient demographics, indication, radiation exposures, access site, procedural duration, dwell time, and complications were identified by the EMR. IVC Filter positioning with measurements of tip to renal vein distance and lateral filter tilt were performed when cavograms or post placement CTs were available for review. Statistical analysis was performed using Stata IC 11.2.
Results: Technical success of the procedure was 100% in both groups. Procedural duration was longer at the bedside lasting 14.5 +/- 10.2 versus 6.7 +/- 6.0 min (p<0.0001). The bedside DR group had a median radiation exposure of 25 mGy (15-35) and the CF group had mean radiation exposure of 256.94 mGy +/- 158.6. There was no significant difference in distance of IVC tip to renal vein (p=0.31), mispositioning (p=0.59), degree of filter tilt (p=0.33), or rate of complications (p=0.65) between the two groups.
Conclusion: IVCF placement at the bedside using DR is comparable to CF with no statistical difference in outcomes based on IVCF positioning, degree of lateral tilt or removal issues. It decreased radiation dose, but with overall increased procedural time.
Keywords: Deep venous thrombosis; Inferior vena cava filters; Pulmonary embolism.
© 2021 Shanghai Journal of Interventional Radiology Press. Publishing services by Elsevier B.V. on behalf of KeAi Communications Co. Ltd.
Conflict of interest statement
None of the authors has a conflict of interest related to this research .
Figures
Similar articles
-
Digital radiograph (DR) guided bedside IVC filter placements in patients with intracranial pressure monitors.J Interv Med. 2021 Aug 19;4(4):208-211. doi: 10.1016/j.jimed.2021.08.005. eCollection 2021 Nov. J Interv Med. 2021. PMID: 35586379 Free PMC article.
-
Role of prophylactic temporary inferior vena cava filters placed at the ICU bedside under intravascular ultrasound guidance in patients with multiple trauma.J Vasc Surg. 2004 Nov;40(5):958-64. doi: 10.1016/j.jvs.2004.07.048. J Vasc Surg. 2004. PMID: 15557911
-
Comparison of Inferior Vena Cava Filters Placed at the Bedside via Intravenous Ultrasound Guidance Versus Fluoroscopic Guidance.Ann Vasc Surg. 2017 Feb;39:250-255. doi: 10.1016/j.avsg.2016.06.013. Epub 2016 Aug 28. Ann Vasc Surg. 2017. PMID: 27581130
-
Comparative analysis of technical success rates and procedural complication rates of bedside inferior vena cava filter placement by intraprocedural imaging modality.J Vasc Surg Venous Lymphat Disord. 2019 Jul;7(4):601-609. doi: 10.1016/j.jvsv.2019.01.061. Epub 2019 May 5. J Vasc Surg Venous Lymphat Disord. 2019. PMID: 31068274
-
Outcomes and associated factors in malpractice litigation involving inferior vena cava filters.J Vasc Surg Venous Lymphat Disord. 2018 Jul;6(4):541-544. doi: 10.1016/j.jvsv.2018.01.016. J Vasc Surg Venous Lymphat Disord. 2018. PMID: 29909860 Review.
Cited by
-
Inferior Vena Cava Filters and Complications: A Systematic Review.Cureus. 2023 Jun 6;15(6):e40038. doi: 10.7759/cureus.40038. eCollection 2023 Jun. Cureus. 2023. PMID: 37287823 Free PMC article. Review.
References
-
- Goldhaber S.Z., Visani L., De Rosa M. Acute pulmonary embolism: clinical outcomes in the international cooperative pulmonary embolism registry (ICOPER) The Lancet (British edition) 1999;353:1386–1389. - PubMed
-
- Dalen J.E., Alpert J.S. Natural history of pulmonary embolism. Prog Cardiovasc Dis. 1975;17:259–270. - PubMed
-
- Caplin D.M., Nikolic B., Kalva S.P. Quality improvement guidelines for the performance of inferior vena cava filter placement for the prevention of pulmonary embolism. J Vasc Intervent Radiol. 2011;22:1499–1506. - PubMed
-
- Kaufman J.A., Kinney T.B., Streiff M.B. Guidelines for the use of retrievable and convertible vena cava filters: report from the society of interventional radiology multidisciplinary consensus conference. Surg Obes Relat Dis. 2006;2:200–212. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials