

Long-term use of immunosuppressive medicines and in-hospital COVID-19 outcomes: a retrospective cohort study using data from the National COVID Cohort Collaborative
- PMID: 34806036
- PMCID: PMC8592562
- DOI: 10.1016/S2665-9913(21)00325-8
Long-term use of immunosuppressive medicines and in-hospital COVID-19 outcomes: a retrospective cohort study using data from the National COVID Cohort Collaborative
Abstract
Background: Many individuals take long-term immunosuppressive medications. We evaluated whether these individuals have worse outcomes when hospitalised with COVID-19 compared with non-immunosuppressed individuals.
Methods: We conducted a retrospective cohort study using data from the National COVID Cohort Collaborative (N3C), the largest longitudinal electronic health record repository of patients in hospital with confirmed or suspected COVID-19 in the USA, between Jan 1, 2020, and June 11, 2021, within 42 health systems. We compared adults with immunosuppressive medications used before admission to adults without long-term immunosuppression. We considered immunosuppression overall, as well as by 15 classes of medication and three broad indications for immunosuppressive medicines. We used Fine and Gray's proportional subdistribution hazards models to estimate the hazard ratio (HR) for the risk of invasive mechanical ventilation, with the competing risk of death. We used Cox proportional hazards models to estimate HRs for in-hospital death. Models were adjusted using doubly robust propensity score methodology.
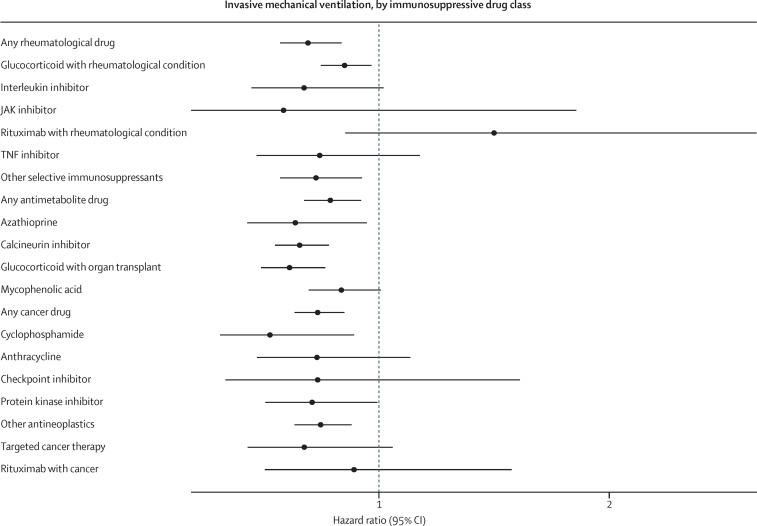
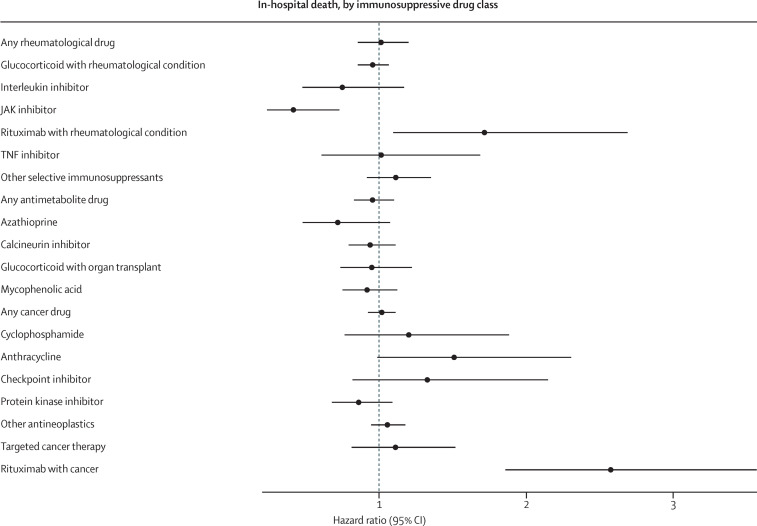
Findings: Among 231 830 potentially eligible adults in the N3C repository who were admitted to hospital with confirmed or suspected COVID-19 during the study period, 222 575 met the inclusion criteria (mean age 59 years [SD 19]; 111 269 [50%] male). The most common comorbidities were diabetes (23%), pulmonary disease (17%), and renal disease (13%). 16 494 (7%) patients had long-term immunosuppression with medications for diverse conditions, including rheumatological disease (33%), solid organ transplant (26%), or cancer (22%). In the propensity score matched cohort (including 12 841 immunosuppressed patients and 29 386 non-immunosuppressed patients), immunosuppression was associated with a reduced risk of invasive ventilation (HR 0·89, 95% CI 0·83-0·96) and there was no overall association between long-term immunosuppression and the risk of in-hospital death. None of the 15 medication classes examined were associated with an increased risk of invasive mechanical ventilation. Although there was no statistically significant association between most drugs and in-hospital death, increases were found with rituximab for rheumatological disease (1·72, 1·10-2·69) and for cancer (2·57, 1·86-3·56). Results were generally consistent across subgroup analyses that considered race and ethnicity or sex, as well as across sensitivity analyses that varied exposure, covariate, and outcome definitions.
Interpretation: Among this cohort, with the exception of rituximab, there was no increased risk of mechanical ventilation or in-hospital death for the rheumatological, antineoplastic, or antimetabolite therapies examined.
Funding: None.
© 2021 Elsevier Ltd. All rights reserved.
Conflict of interest statement
RBM reports grants and other fees from Vitaeris/CSL Behring; other fees from the American Journal of Transplantation; and grants from Mallinckrodt, CSL Behring, Transplant Genomics, and Quark Phamaceuticals, outside the submitted work. RCP reports grants from Trasher Foundation and investigator-sponsored studies from Merck, outside the submitted work. JSi reports consulting fees from Crealta/Horizon, Medisys, Fidia, PK Med, Two Labs, Adept Field Solutions, Clinical Care Options, Clearview Healthcare Partners, Putnam Associates, Focus Forward, Navigant Consulting, Spherix, MedIQ, Jupiter Life Science, UBM, Trio Health, Medscape, WebMD, and Practice Point Communications, the National Institutes of Health, and the American College of Rheumatology; is on the speaker's bureau of Simply Speaking; receives support from OMERACT to attend their biennial meeting; serves as a member of the US Food and Drug Administration (FDA) Arthritis Advisory Committee; serves as the Chair of the Veterans Affairs Rheumatology Field Advisory Committee, is the editor and director of the UAB Cochrane; owns stock options in TPT Global Tech, Vaxart Pharmaceuticals, and Charlotte's Web Holdings, and previously owned stock options in Amarin, Viking, and Moderna Pharmaceuticals, outside the submitted work. PGA reports consulting fees from EMD Serono; has participated on a data safety monitoring board or advisory board for Humanigen; and has personal stock or stock options with Johnson and Johnson. HBM reports investigator initiated research grants from Bristol Myers Squibb. GCA is a current member and past chair of the FDA Peripheral and Central Nervous System Advisory Committee, is a co-founding principal and equity holder in Monument Analytics, a health care consultancy with clients in the life sciences industry as well as plaintiffs in opioid litigation, and is a past member of OptumRx's National Pharmacy and Therapeutics Committee. BTG is a member of the FDA Pulmonary and Asthma Drug Advisory Committee, has received speaking fees from Gilead Sciences, and consulting fees from Janssen Research and Development. All other authors declare no competing interests.
Figures
References
-
- Johns Hopkins University & Medicine Coronavirus resource center. https://coronavirus.jhu.edu
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
