

Lung cancer mortality reduction by LDCT screening: UKLS randomised trial results and international meta-analysis
- PMID: 34806061
- PMCID: PMC8589726
- DOI: 10.1016/j.lanepe.2021.100179
Lung cancer mortality reduction by LDCT screening: UKLS randomised trial results and international meta-analysis
Abstract
Background: The NLST reported a significant 20% reduction in lung cancer mortality with three annual low-dose CT (LDCT) screens and the Dutch-Belgian NELSON trial indicates a similar reduction. We present the results of the UKLS trial.
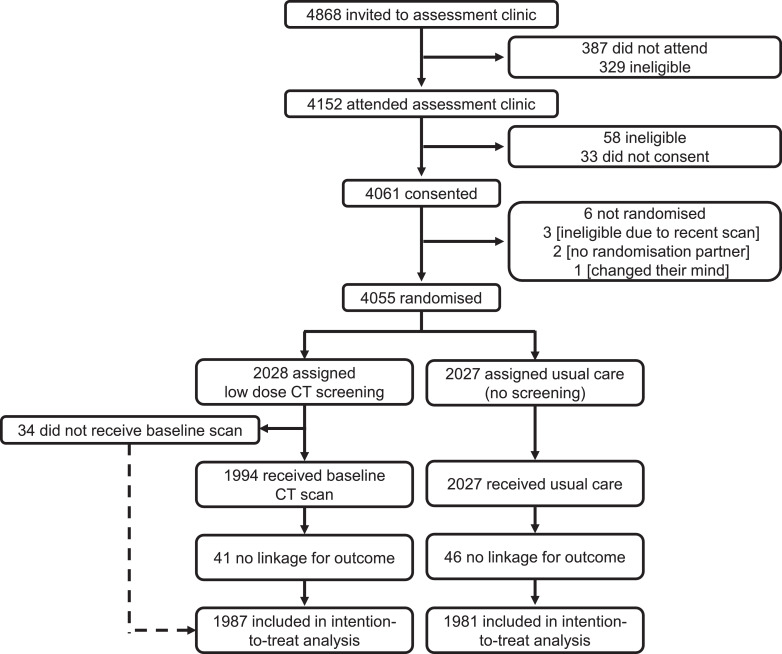
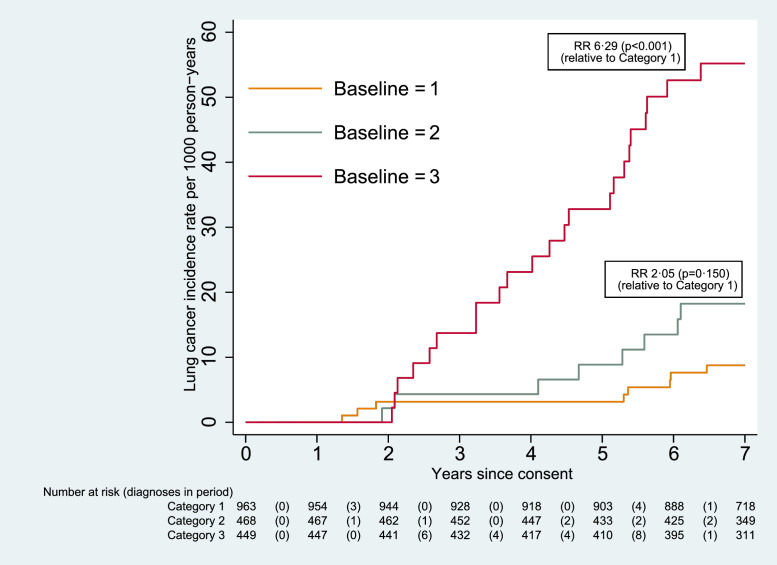
Methods: From October 2011 to February 2013, we randomly allocated 4 055 participants to either a single invitation to screening with LDCT or to no screening (usual care). Eligible participants (aged 50-75) had a risk score (LLPv2) ≥ 4.5% of developing lung cancer over five years. Data were collected on lung cancer cases to 31 December 2019 and deaths to 29 February 2020 through linkage to national registries. The primary outcome was mortality due to lung cancer. We included our results in a random-effects meta-analysis to provide a synthesis of the latest randomised trial evidence.
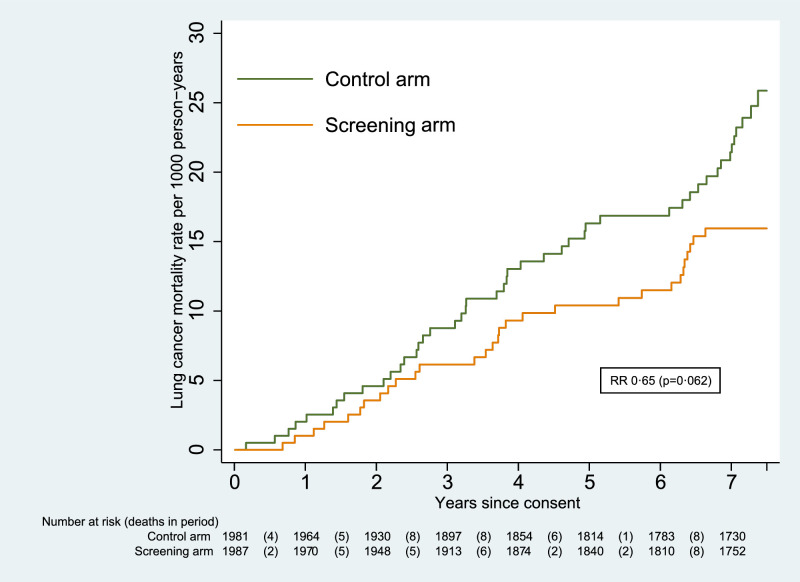
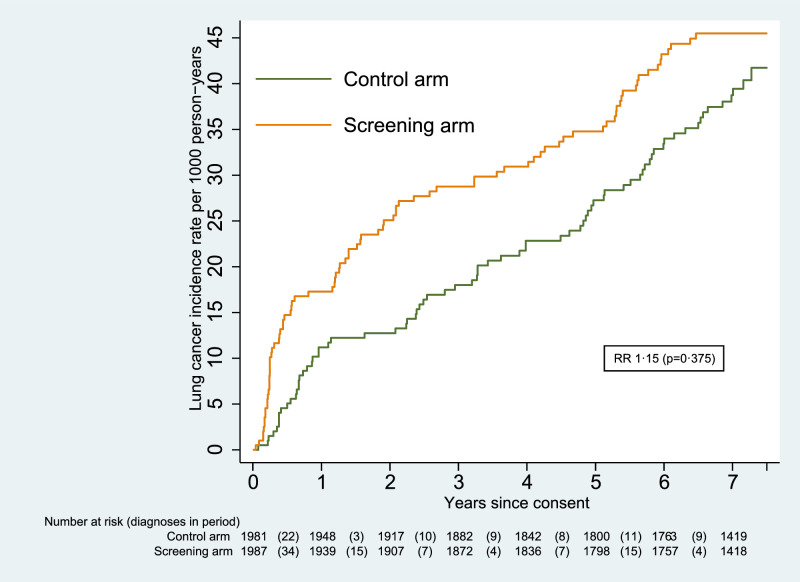
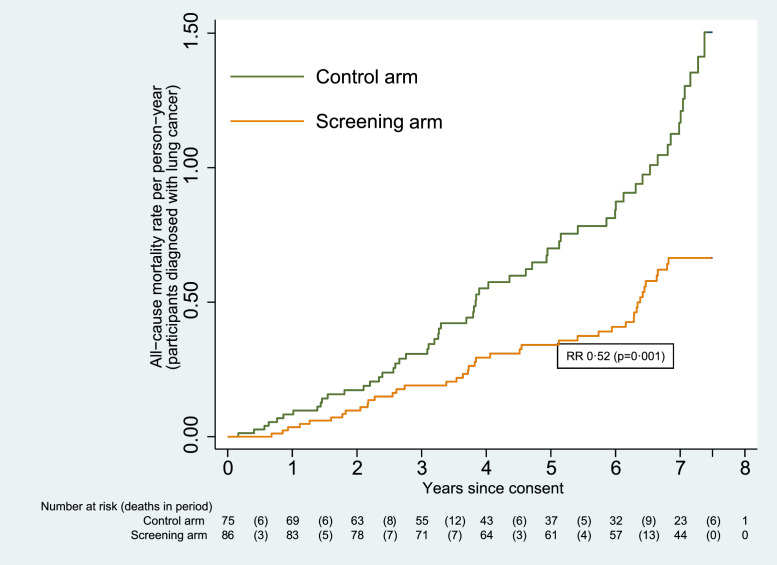
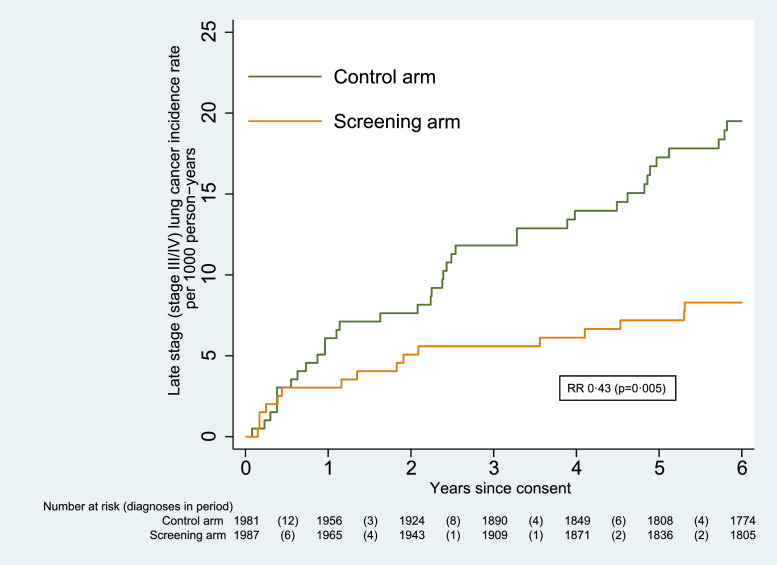
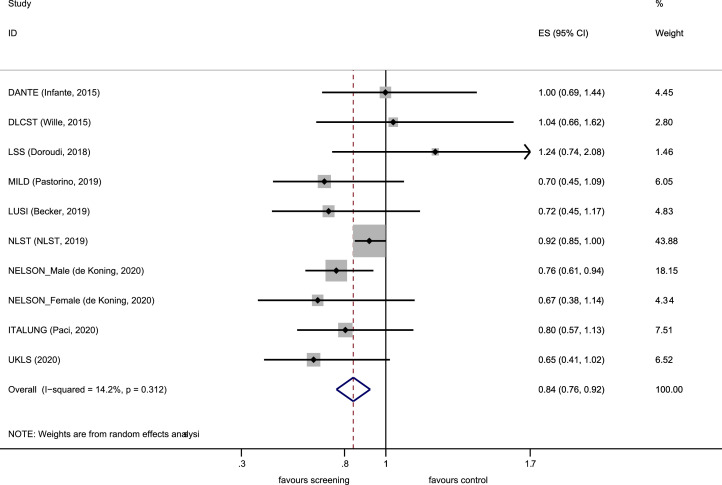
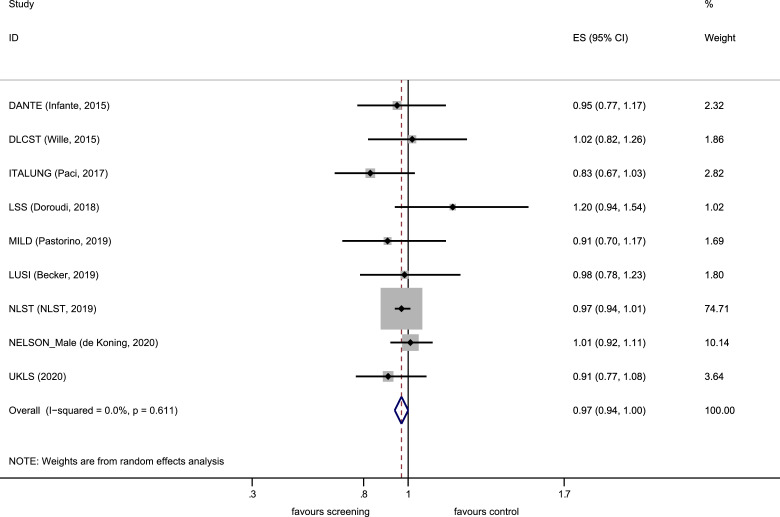
Findings: 1 987 participants in the intervention and 1 981 in the usual care arms were followed for a median of 7.3 years (IQR 7.1-7.6), 86 cancers were diagnosed in the LDCT arm and 75 in the control arm. 30 lung cancer deaths were reported in the screening arm, 46 in the control arm, (relative rate 0.65 [95% CI 0.41-1.02]; p=0.062). The meta-analysis indicated a significant reduction in lung cancer mortality with a pooled overall relative rate of 0.84 (95% CI 0.76-0.92) from nine eligible trials.
Interpretation: The UKLS trial of single LDCT indicates a reduction of lung cancer death of similar magnitude to the NELSON and NLST trials and was included in a meta-analysis of nine randomised trials which provides unequivocal support for lung cancer screening in identified risk groups.
Funding: NIHR Health Technology Assessment programme; NIHR Policy Research programme; Roy Castle Lung Cancer Foundation.
Keywords: CT Screening; Lung Cancer; Lung Cancer Mortality; Meta-analysis.
© 2021 The Authors.
Conflict of interest statement
JKF has received fees from AstraZeneca (Speaker's Bureau) and advisory boards of Epigenomics; NUCLEIX Ltd. AstraZeneca, iDNA; Grant Support: Janssen Research & Development, LLC. RCR is on the advisory boards of AstraZeneca and Roche. DRB has received speaker remuneration from AstraZeneca, Roche, MSD, BMS, Johnson and Johnson. KB has received personal fees from Astra Zeneca outside the submitted work. TE receives research support from AstraZeneca, Bayer, Pfizer; is employed by Roche (from March 2020) and was employed by AstraZeneca (to March 2020) and has stock in AstraZeneca and Roche; is a trustee of Macmillan Cancer Support. AN has current grants and contracts with BRC, DART; Honoraria Aidence BV, AstraZeneca; Support from BLF, and as the clinical lead for NTLHC. No competing interests from all other co-authors.
Figures
References
-
- Marcus P.M., Bergstralh E.J., Fagerstrom R.M., et al. Lung cancer mortality in the mayo lung project: impact of extended follow-up. J Natl Cancer Inst. 2000;92(16):1308–1316. - PubMed
-
- Frost J.K., Ball W.C., Levin M.L., et al. Early lung cancer detection: results of the initial (prevalence) radiologic and cytologic screening in the Johns Hopkins study. Am Rev Respir Dis. 1984;130(4):549–554. - PubMed
-
- Kaneko M., Eguchi K., Ohmatsu H., et al. Peripheral lung cancer: screening and detection with low-dose spiral CT versus radiography. Radiology. 1996;201(3):798–802. - PubMed
-
- Henschke C.I., McCauley D.I., Yankelevitz D.F., et al. Early lung cancer action project: overall design and findings from baseline screening. Lancet. 1999;354(9173):99–105. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
