

Antithrombotic therapy in patients with liver disease: population-based insights on variations in prescribing trends, adherence, persistence and impact on stroke and bleeding
- PMID: 34806071
- PMCID: PMC8589727
- DOI: 10.1016/j.lanepe.2021.100222
Antithrombotic therapy in patients with liver disease: population-based insights on variations in prescribing trends, adherence, persistence and impact on stroke and bleeding
Abstract
Background: Patients with liver disease have complex haemostasis and due to such contraindications, landmark randomised controlled trials investigating antithrombotic medicines have often excluded these patients. As a result, there has been limited consensus on the safety, efficacy and monitoring practices of anticoagulant and antiplatelet therapy in patients with liver disease. This study aims to investigate prescribing prevalence, adherence, persistence and impact of adherence on bleeding and stroke risk in people with and without liver disease taking anticoagulants and antiplatelets.
Methods: We employed a population-based cohort consisting of person-level linked records from primary care, secondary care and the death registry. The cohort consisted of 3,929,596 adults aged ≥ 30 years during the study period of 1998 to 2020 and registered with an NHS general practitioner in England. The primary outcome was prescribing prevalence, adherence to and persistence with anticoagulant and antiplatelet therapy comparing patients with and without liver disease. Risk factors for non-adherence and non-persistence were analysed using multivariable logistic regression and Cox regression. Impact of adherence on bleeding and ischaemic stroke was assessed.
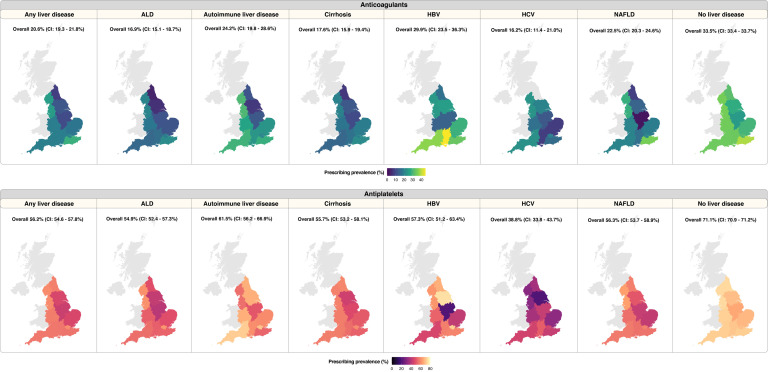
Findings: Among patients with any of the six liver diseases (ALD, autoimmune liver disease, cirrhosis, HBV, HCV and NAFLD), we identified 4,237 individuals with incident atrial fibrillation (indication for anticoagulants) and 4,929 individuals with incident myocardial infarction, transient ischaemic attack, unstable angina or peripheral arterial disease (indication for antiplatelets). Among patients without liver disease, 321,510 and 386,643 individuals were identified as having indications for anticoagulant and antiplatelet therapy, respectively. Among drug-naïve individuals, prescribing prevalence was lower in patients with liver disease compared with individuals without liver disease: anticoagulants (20.6% [806/3,921] vs. 33.5% [103,222/307,877]) and antiplatelets (56.2% [2,207/3,927] vs. 71.1% [249,258/350,803]). Primary non-adherence rates (stopping after one prescription) were higher in patients with liver disease, compared with those without liver disease: anticoagulants (7.9% [64/806] vs. 4.7% [4,841/103,222]) and antiplatelets (6.2% [137/2,207] vs. 4.4% [10,993/249,258]). Among individuals who were not primary non-adherent and had at least 12 months of follow-up, patients with liver disease however had a higher one-year adherence rate: anticoagulants (33.1% [208/628] vs. 29.4% [26,615/90,569]) and antiplatelets (40.9% [743/1,818] vs. 34.4% [76,834/223,154]). Likelihood of non-adherence was lower in apixaban and rivaroxaban (relative to warfarin) and lower in clopidogrel (relative to aspirin). Increased comorbidity burden (by CHA2DS2VASc score) was associated with decreased risk of non-adherence and non-persistence with anticoagulants. Overall rates of 'non-adherent, non-persistent' were highest in warfarin (compared with apixaban and rivaroxaban) and aspirin (compared with clopidogrel or dipyridamole) in patients with and without liver disease. Among patients without liver disease, not taking antithrombotic medications for >3 months was associated with a higher risk of stroke, however, adherence to these medications was also associated with a small increase in risk of bleeding. Patients with liver disease (when compared with those without liver disease) had higher risks of stroke, especially when they stopped taking antiplatelets for >3 months. Patients with liver disease who were adherent to antiplatelets, however, had a higher risk of bleeding compared with patients without liver disease.
Interpretation: Use of antithrombotic medicines in patients with and without liver disease is suboptimal with heterogeneity across medicines. As patients with liver disease are excluded from major randomised trials for these drugs, our results provide real-world evidence that may inform medicine optimisation strategies. We outline challenges and opportunities for tackling non-adherence, which begins with understanding patients' views of medicines to help them make informed decisions about appropriate use.
Funding: AGL is supported by funding from the Wellcome Trust (204841/Z/16/Z), National Institute for Health Research (NIHR) University College London Hospitals Biomedical Research Centre (BRC714/HI/RW/101440), NIHR Great Ormond Street Hospital Biomedical Research Centre (19RX02), the Health Data Research UK Better Care Catalyst Award (CFC0125) and the Academy of Medical Sciences (SBF006\1084). The funders have no role in the writing of the manuscript or the decision to submit it for publication.
Keywords: Antiplatelets; adherence; anticoagulants; bleeding; liver disease; persistence; prescribing pattern; stroke.
© 2021 The Author(s).
Conflict of interest statement
None declared.
Figures


References
-
- Younossi ZM, Koenig AB, Abdelatif D, Fazel Y, Henry L, Wymer M. Global epidemiology of nonalcoholic fatty liver disease—meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology. 2016;64:73–84. - PubMed
-
- Estes C, Anstee QM, Arias-Loste MT, et al. Modeling nafld disease burden in china, france, germany, italy, japan, spain, united kingdom, and united states for the period 2016–2030. J Hepatol. 2018;69:896–904. - PubMed
-
- Lazarus JV, Ekstedt M, Marchesini G, et al. A cross-sectional study of the public health response to non-alcoholic fatty liver disease in Europe. J Hepatol. 2020;72:14–24. - PubMed
-
- Stepanova M, Younossi ZM. Independent association between nonalcoholic fatty liver disease and cardiovascular disease in the US population. Clin Gastroenterol Hepatol. 2012;10:646–650. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
