

Brain metastases: the role of clinical imaging
- PMID: 34808072
- PMCID: PMC8822566
- DOI: 10.1259/bjr.20210944
Brain metastases: the role of clinical imaging
Abstract
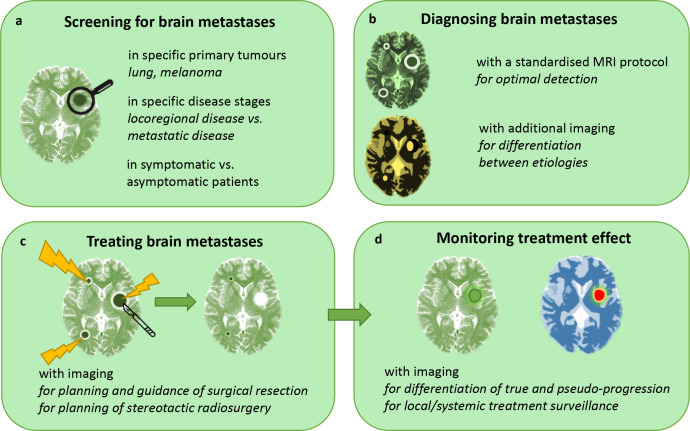
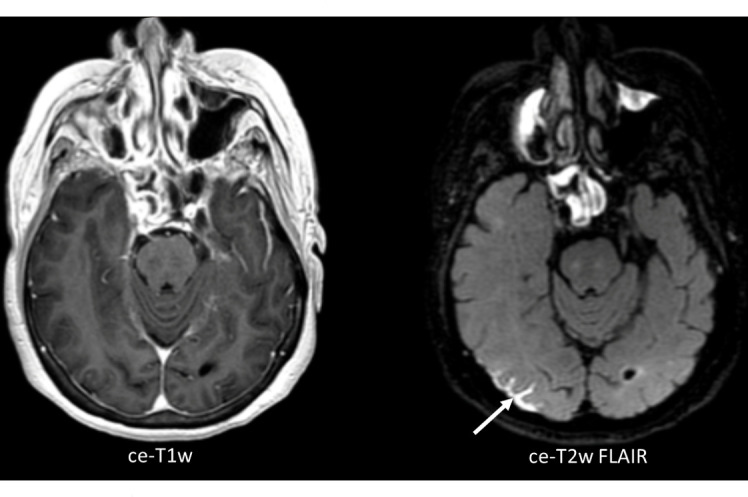
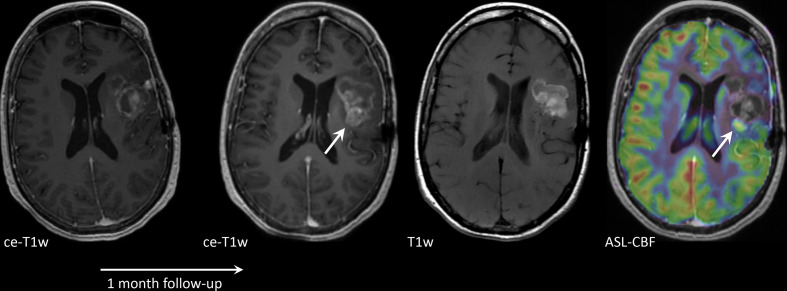
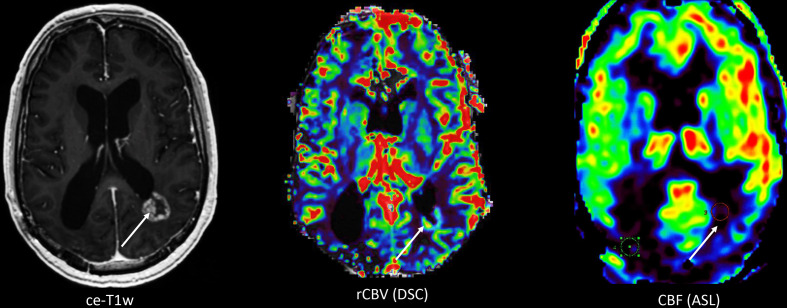
Imaging of brain metastases (BMs) has advanced greatly over the past decade. In this review, we discuss the main challenges that BMs pose in clinical practice and describe the role of imaging.Firstly, we describe the increased incidence of BMs of different primary tumours and the rationale for screening. A challenge lies in selecting the right patients for screening: not all cancer patients develop BMs in their disease course.Secondly, we discuss the imaging techniques to detect BMs. A three-dimensional (3D) T1W MRI sequence is the golden standard for BM detection, but additional anatomical (susceptibility weighted imaging, diffusion weighted imaging), functional (perfusion MRI) and metabolic (MR spectroscopy, positron emission tomography) information can help to differentiate BMs from other intracranial aetiologies.Thirdly, we describe the role of imaging before, during and after treatment of BMs. For surgical resection, imaging is used to select surgical patients, but also to assist intraoperatively (neuronavigation, fluorescence-guided surgery, ultrasound). For treatment planning of stereotactic radiosurgery, MRI is combined with CT. For surveillance after both local and systemic therapies, conventional MRI is used. However, advanced imaging is increasingly performed to distinguish true tumour progression from pseudoprogression.FInally, future perspectives are discussed, including radiomics, new biomarkers, new endogenous contrast agents and theranostics.
Figures
References
-
- Goldberg SB, Gettinger SN, Mahajan A, Chiang AC, Herbst RS, Sznol M, et al. . Pembrolizumab for patients with melanoma or non-small-cell lung cancer and untreated brain metastases: early analysis of a non-randomised, open-label, phase 2 trial. Lancet Oncol 2016; 17: 976–83. doi: 10.1016/S1470-2045(16)30053-5 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
