

Updates on the ketogenic diet therapy for pediatric epilepsy
- PMID: 34808422
- PMCID: PMC9133260
- DOI: 10.1016/j.bj.2021.11.003
Updates on the ketogenic diet therapy for pediatric epilepsy
Abstract
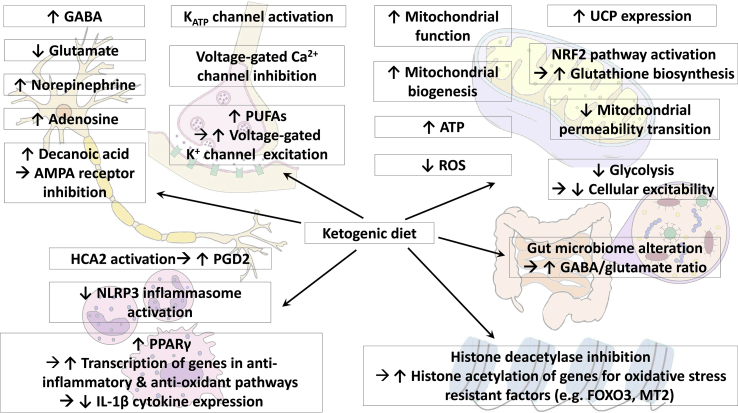
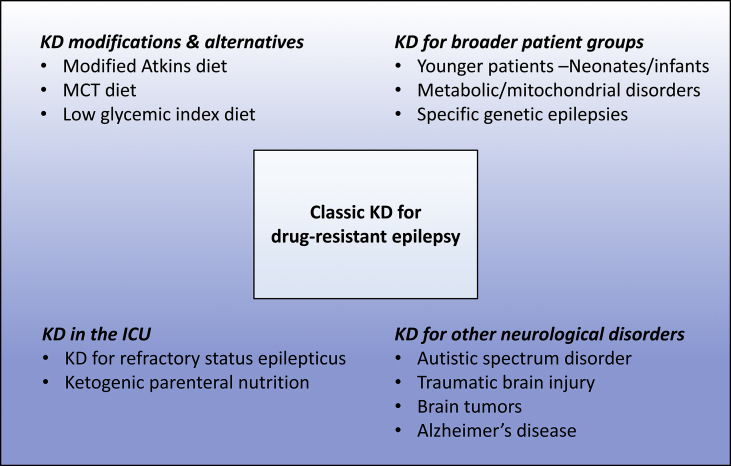
The ketogenic diet (KD) is a high-fat, low-carbohydrate diet, in which fat, instead of glucose, acts as a major energy source through the production of ketone bodies. The KD was formally introduced in 1921 to mimic the biochemical changes associated with fasting and gained recognition as a potent treatment for pediatric epilepsy in the mid-1990s. Recent clinical and scientific knowledge supports the use of the KD in drug-resistant epilepsy patients for its anti-seizure efficacy, safety, and tolerability. The KD is also receiving growing attention as a potential treatment option for other neurological disorders. This article will review on the recent updates on the KD, focusing on its mechanisms of action, its alternatives, expansion on its use in terms of age groups and different regions in the world, and future issues.
Keywords: Epilepsy; Ketogenic diet; Pediatric.
Copyright © 2021 Chang Gung University. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Conflicts of interest There is no competing interest among the authors.
Figures
References
-
- Wheless J.W. History of the ketogenic diet. Epilepsia. 2008;49 Suppl 8:3–5. - PubMed
-
- Guelpa G., Marie A. La lutte contre l'epilepsie par la desintoxication et par la reeducation alimentaire. Rev Ther Med Chir. 1911;78:8–13.
-
- Wilder R.M. The effects of ketonemia on the course of epilepsy. Mayo Clin Proc. 1921;2:307–308.
-
- Martin K., Jackson C.F., Levy R.G., Cooper P.N. Ketogenic diet and other dietary treatments for epilepsy. Cochrane Database Syst Rev. 2016;2 Update in: Cochrane Database Syst Rev 2018;11:CD001903. - PubMed
-
- Kossoff E.H., Zupec-Kania B.A., Amark P.E., Ballaban-Gil K.R., Christina Bergqvist A.G., Blackford R., et al. Optimal clinical management of children receiving the ketogenic diet: recommendations of the International Ketogenic Diet Study Group. Epilepsia. 2009;50:304–317. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
