

Chlamydia pneumoniae-associated pleuropericarditis: a case report and systematic review of the literature
- PMID: 34809625
- PMCID: PMC8607726
- DOI: 10.1186/s12890-021-01743-9
Chlamydia pneumoniae-associated pleuropericarditis: a case report and systematic review of the literature
Abstract
Background: Chlamydia pneumoniae is a common cause of atypical community acquired pneumonia (CAP). The diagnostic approach of chlamydial infections remains a challenge. Diagnosis of delayed chlamydial-associated complications, involving complex autoimmune pathophysiological mechanisms, is still more challenging. C. pneumoniae-related cardiac complications have been rarely reported, including cases of endocarditis, myocarditis and pericarditis.
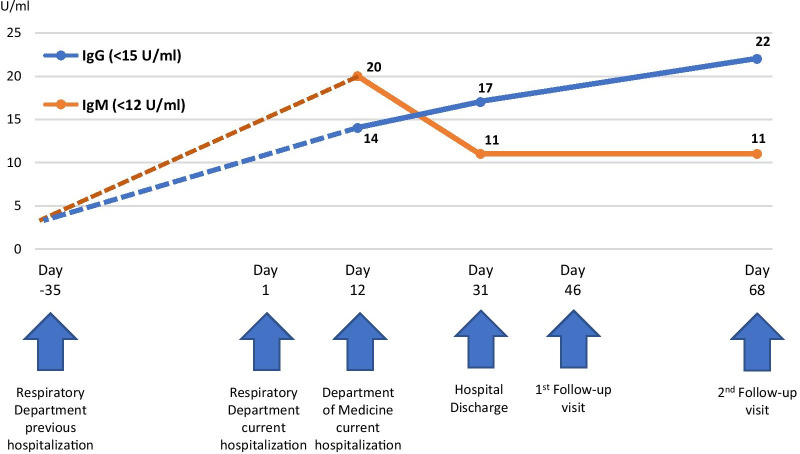
Case presentation: A 40-year old female was hospitalized for pleuropericarditis following lower respiratory tract infection. The patient had been hospitalized for CAP (fever, dyspnea, chest X-ray positive for consolidation on the left upper lobe) 5 weeks ago and had received ceftriaxone and moxifloxacin. Four weeks after her discharge, the patient presented with fever, shortness of breath and pleuritic chest pain and was readmitted because of pericardial and bilateral pleural effusions (mainly left). The patient did not improve on antibiotics and sequential introduction of colchicine and methylprednisolone was performed. The patient presented impressive clinical and laboratory response. Several laboratory and clinical assessments failed to demonstrate any etiological factor for serositis. Chlamydial IgM and IgG antibodies were positive and serial measurements showed increasing kinetics for IgG. Gold standard polymerase chain reaction of respiratory tract samples was not feasible but possibly would not have provided any additional information since CAP occurred 5 weeks ago. The patient was discharged under colchicine and tapered methylprednisolone course. During regular clinic visits, she remained in good clinical condition without pericardial and pleural effusions relapse.
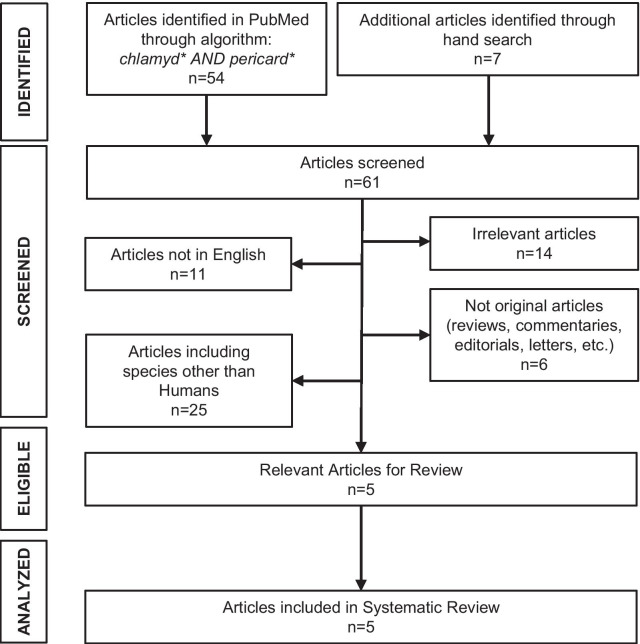
Conclusions: C. pneumoniae should be considered as possible pathogen in case of pleuritis and/or pericarditis during or after a lower respiratory tract infection. In a systematic review of the literature only five cases of C. pneumoniae associated pericarditis were identified. Exact mechanisms of cardiovascular damage have not yet been defined, yet autoimmune pathways might be implicated.
Keywords: Antigenic mimicry; Chlamydia pneumonia; Community acquired pneumonia; Pericarditis; Pleuritis; Pleuropericarditis; Serositis.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Acute hemorrhagic pericarditis in a child with pneumonia due to Chlamydophila pneumoniae.J Clin Microbiol. 2005 Jan;43(1):520-2. doi: 10.1128/JCM.43.1.520-522.2005. J Clin Microbiol. 2005. PMID: 15635034 Free PMC article.
-
Acute haemorrhagic pericarditis: an unusual presentation of Chlamydophila pneumoniae pneumonia infection.Paediatr Int Child Health. 2020 Aug;40(3):207-210. doi: 10.1080/20469047.2020.1728163. Epub 2020 Feb 13. Paediatr Int Child Health. 2020. PMID: 32052706
-
[Acute pericarditis as an organic manifestation of the acute infection Chlamydia pneumoniae].Vnitr Lek. 2008 Sep;54(9):866-70. Vnitr Lek. 2008. PMID: 18924348 Czech.
-
Chlamydial infections of the heart.Eur J Clin Microbiol Infect Dis. 1992 Oct;11(10):885-93. doi: 10.1007/BF01962368. Eur J Clin Microbiol Infect Dis. 1992. PMID: 1486883 Review.
-
Where is Chlamydophila pneumoniae pneumonia?Respir Investig. 2020 Sep;58(5):336-343. doi: 10.1016/j.resinv.2020.06.002. Epub 2020 Jul 20. Respir Investig. 2020. PMID: 32703757
Cited by
-
Pleural Effusions and Pericarditis: A Retrospective Cohort Study of Patients Undergoing Cardiac Magnetic Resonance Imaging.Cureus. 2022 Mar 29;14(3):e23599. doi: 10.7759/cureus.23599. eCollection 2022 Mar. Cureus. 2022. PMID: 35494953 Free PMC article.
-
Chlamydophila pneumoniae-associated community-acquired pneumonia in paediatric patients of a tertiary care hospital in Mexico: molecular diagnostic and clinical insights.Sci Rep. 2023 Dec 6;13(1):21477. doi: 10.1038/s41598-023-48701-5. Sci Rep. 2023. PMID: 38052876 Free PMC article.
References
-
- Gnarpe H, Gnarpe J, Gästrin B, Hallander H. Chlamydia pneumoniae and myocarditis. Scand J Infect Dis Suppl. 1997;104:50–52. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
