

Dysmetabolism, Diabetes and Clinical Outcomes in Patients Cured of Chronic Hepatitis C: A Real-Life Cohort Study
- PMID: 34811949
- PMCID: PMC8948549
- DOI: 10.1002/hep4.1851
Dysmetabolism, Diabetes and Clinical Outcomes in Patients Cured of Chronic Hepatitis C: A Real-Life Cohort Study
Abstract
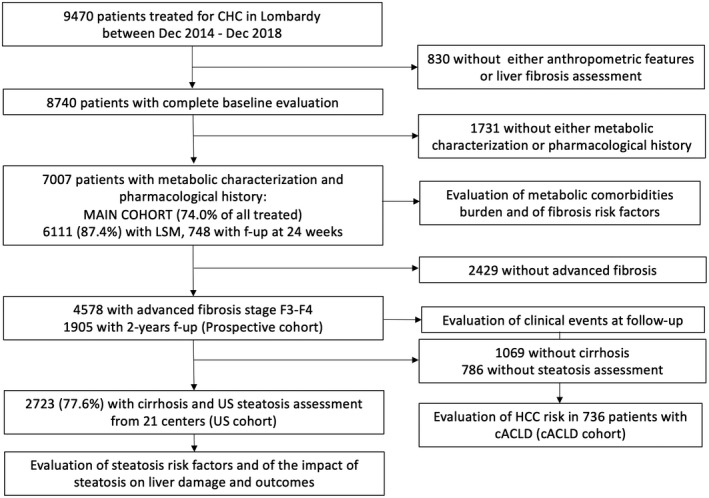
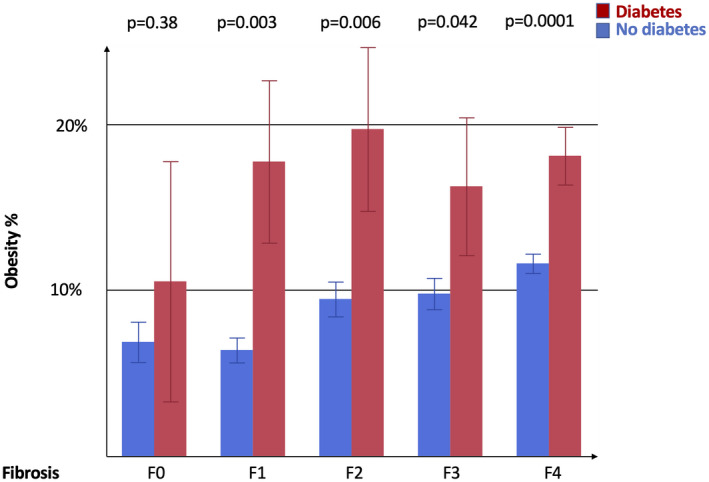
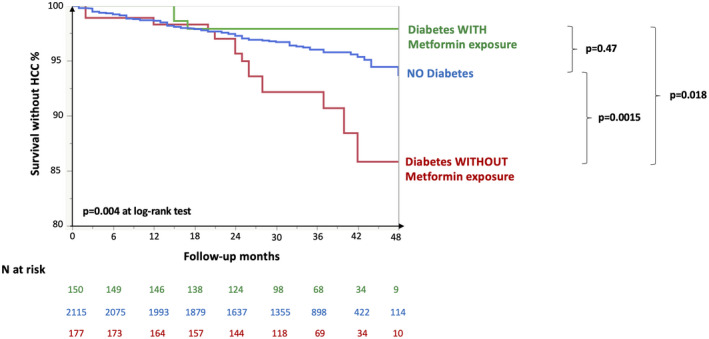
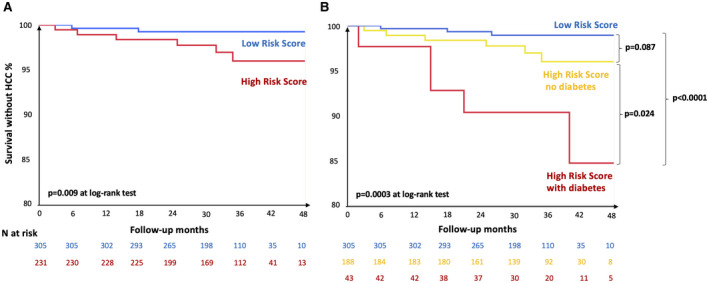
The aim of this study was to examine the impact of features of dysmetabolism on liver disease severity, evolution, and clinical outcomes in a real-life cohort of patients treated with direct acting antivirals for chronic hepatitis C virus (HCV) infection. To this end, we considered 7,007 patients treated between 2014 and 2018, 65.3% with advanced fibrosis, of whom 97.7% achieved viral eradication (NAVIGATORE-Lombardia registry). In a subset (n = 748), liver stiffness measurement (LSM) was available at baseline and follow-up. Higher body mass index (BMI; odds ratio [OR] 1.06 per kg/m2 , 1.03-1.09) and diabetes (OR 2.01 [1.65-2.46]) were independently associated with advanced fibrosis at baseline, whereas statin use was protective (OR 0.46 [0.35-0.60]; P < 0.0001 for all). The impact of BMI was greater in those without diabetes (P = 0.003). Diabetes was independently associated with less pronounced LSM improvement after viral eradication (P = 0.001) and in patients with advanced fibrosis was an independent predictor of the most frequent clinical events, namely de novo hepatocellular carcinoma (HCC; hazard ratio [HR] 2.09 [1.20-3.63]; P = 0.009) and cardiovascular events (HR 2.73 [1.16-6.43]; P = 0.021). Metformin showed a protective association against HCC (HR 0.32 [0.11-0.96]; P = 0.043), which was confirmed after adjustment for propensity score (P = 0.038). Diabetes diagnosis further refined HCC prediction in patients with compensated advanced chronic liver disease at high baseline risk (P = 0.024). Conclusion: Metabolic comorbidities were associated with advanced liver fibrosis at baseline, whereas statins were protective. In patients with advanced fibrosis, diabetes increased the risk of de novo HCC and of cardiovascular events. Optimization of metabolic comorbidities treatment by a multi-disciplinary management approach may improve cardiovascular and possibly liver-related outcomes.
© 2021 The Authors. Hepatology Communications published by Wiley Periodicals LLC on behalf of American Association for the Study of Liver Diseases.
Figures
References
-
- European Association for the Study of the Liver . EASL recommendations on treatment of hepatitis C 2018. J Hepatol 2018;69:461‐511. - PubMed
-
- Goldberg D, Ditah IC, Saeian K, Lalehzari M, Aronsohn A, Gorospe EC, et al. Changes in the prevalence of hepatitis C virus infection, nonalcoholic steatohepatitis, and alcoholic liver disease among patients with cirrhosis or liver failure on the waitlist for liver transplantation. Gastroenterology 2017;152:1090‐1099.e1091. - PMC - PubMed
-
- Di Marco V, Calvaruso V, Ferraro D, Bavetta MG, Cabibbo G, Conte E, et al. Effects of eradicating hepatitis C virus infection in patients with cirrhosis differ with stage of portal hypertension. Gastroenterology 2016;151:130‐139.e132. - PubMed
-
- Aghemo A, Prati GM, Rumi MG, Soffredini R, D'Ambrosio R, Orsi E, et al. Sustained virological response prevents the development of insulin resistance in patients with chronic hepatitis C. Hepatology 2012;56:1681‐1687. - PubMed
-
- D'Ambrosio R, Aghemo A, Rumi MG, Ronchi G, Donato MF, Paradis V, et al. A morphometric and immunohistochemical study to assess the benefit of a sustained virological response in hepatitis C virus patients with cirrhosis. Hepatology 2012;56:532‐543. - PubMed
