

COVID-19 Artificial Intelligence Diagnosis Using Only Cough Recordings
- PMID: 34812418
- PMCID: PMC8545024
- DOI: 10.1109/OJEMB.2020.3026928
COVID-19 Artificial Intelligence Diagnosis Using Only Cough Recordings
Abstract
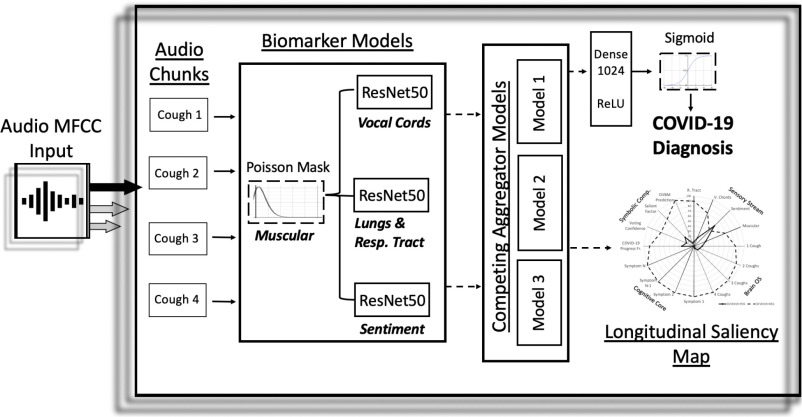
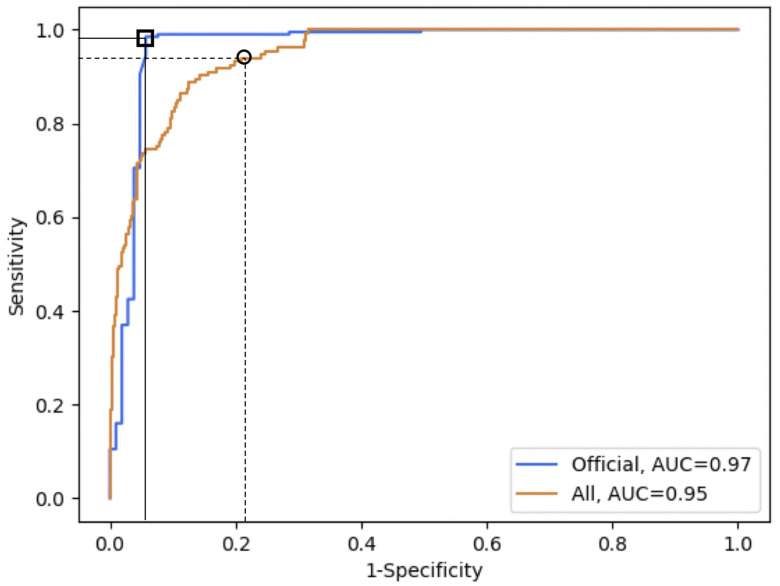
Goal: We hypothesized that COVID-19 subjects, especially including asymptomatics, could be accurately discriminated only from a forced-cough cell phone recording using Artificial Intelligence. To train our MIT Open Voice model we built a data collection pipeline of COVID-19 cough recordings through our website (opensigma.mit.edu) between April and May 2020 and created the largest audio COVID-19 cough balanced dataset reported to date with 5,320 subjects. Methods: We developed an AI speech processing framework that leverages acoustic biomarker feature extractors to pre-screen for COVID-19 from cough recordings, and provide a personalized patient saliency map to longitudinally monitor patients in real-time, non-invasively, and at essentially zero variable cost. Cough recordings are transformed with Mel Frequency Cepstral Coefficient and inputted into a Convolutional Neural Network (CNN) based architecture made up of one Poisson biomarker layer and 3 pre-trained ResNet50's in parallel, outputting a binary pre-screening diagnostic. Our CNN-based models have been trained on 4256 subjects and tested on the remaining 1064 subjects of our dataset. Transfer learning was used to learn biomarker features on larger datasets, previously successfully tested in our Lab on Alzheimer's, which significantly improves the COVID-19 discrimination accuracy of our architecture. Results: When validated with subjects diagnosed using an official test, the model achieves COVID-19 sensitivity of 98.5% with a specificity of 94.2% (AUC: 0.97). For asymptomatic subjects it achieves sensitivity of 100% with a specificity of 83.2%. Conclusions: AI techniques can produce a free, non-invasive, real-time, any-time, instantly distributable, large-scale COVID-19 asymptomatic screening tool to augment current approaches in containing the spread of COVID-19. Practical use cases could be for daily screening of students, workers, and public as schools, jobs, and transport reopen, or for pool testing to quickly alert of outbreaks in groups. General speech biomarkers may exist that cover several disease categories, as we demonstrated using the same ones for COVID-19 and Alzheimer's.
Keywords: AI diagnostics; COVID-19 screening; convolutional neural networks; deep learning; speech recognition.
This work is licensed under a Creative Commons Attribution 4.0 License. For more information, see https://creativecommons.org/licenses/by/4.0/.
Figures
References
-
- Barro R. J., Ursua J. F., and Weng J., “The coronavirus and the great influenza pandemic: Lessons from the “spanish flu” for the coronavirus's potential effects on mortality and economic activity,” Nat. Bur. Econ. Res., Cambridge, MA, USA, Tech. Rep. w26866, 2020.
-
- “Why your coronavirus test could cost 23 – or 2,315,” Jun. 2020. [Online]. Available: https://www.advisory.com/dailybriefing/2020/06/17/covid-test-cost
-
- Salathe M. et al. , “Covid-19 epidemic in Switzerland: On the importance of testing, contact tracing and isolation,” Swiss Med. Weekly, vol. 150, no. 11-12, 2020, Paper w20225. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
