

Ten months of temporal variation in the clinical journey of hospitalised patients with COVID-19: An observational cohort
- PMID: 34812731
- PMCID: PMC8791638
- DOI: 10.7554/eLife.70970
Ten months of temporal variation in the clinical journey of hospitalised patients with COVID-19: An observational cohort
Abstract
Background: There is potentially considerable variation in the nature and duration of the care provided to hospitalised patients during an infectious disease epidemic or pandemic. Improvements in care and clinician confidence may shorten the time spent as an inpatient, or the need for admission to an intensive care unit (ICU) or high dependency unit (HDU). On the other hand, limited resources at times of high demand may lead to rationing. Nevertheless, these variables may be used as static proxies for disease severity, as outcome measures for trials, and to inform planning and logistics.
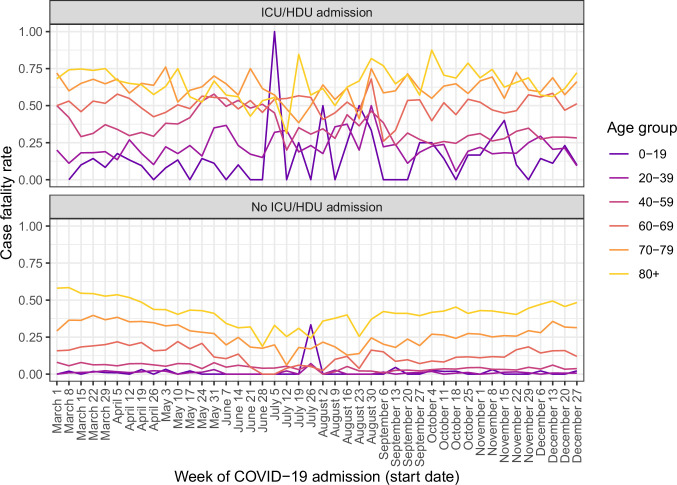
Methods: We investigate these time trends in an extremely large international cohort of 142,540 patients hospitalised with COVID-19. Investigated are: time from symptom onset to hospital admission, probability of ICU/HDU admission, time from hospital admission to ICU/HDU admission, hospital case fatality ratio (hCFR) and total length of hospital stay.
Results: Time from onset to admission showed a rapid decline during the first months of the pandemic followed by peaks during August/September and December 2020. ICU/HDU admission was more frequent from June to August. The hCFR was lowest from June to August. Raw numbers for overall hospital stay showed little variation, but there is clear decline in time to discharge for ICU/HDU survivors.
Conclusions: Our results establish that variables of these kinds have limitations when used as outcome measures in a rapidly evolving situation.
Funding: This work was supported by the UK Foreign, Commonwealth and Development Office and Wellcome [215091/Z/18/Z] and the Bill & Melinda Gates Foundation [OPP1209135]. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Keywords: COVID-19; ICU; SARS-CoV-2; epidemiology; global health; hospitalisation; human; medicine; viruses.
© 2021, ISARIC Clinical Characterisation Group et al.
Conflict of interest statement
MH, JB, GC, BC, AD, ED, CD, JD, ME, CK, LM, MP, JW, PH, AR, PO No competing interests declared
Figures









References
-
- Bell LC, Norris-Grey C, Luintel A, Bidwell G, Lanham D, Marks M, Baruah T, O’Shea L, Heightman M, Logan S, University College London Hospitals COVID response team Implementation and evaluation of a COVID-19 rapid follow-up service for patients discharged from the emergency department. Clinical Medicine. 2021;21:e57–e62. doi: 10.7861/clinmed.2020-0816. - DOI - PMC - PubMed
-
- Choi H-G, Wee JH, Kim SY, Kim J-H, Il Kim H, Park J-Y, Park S, Il Hwang Y, Jang SH, Jung K-S. Association between asthma and clinical mortality/morbidity in COVID-19 patients using clinical epidemiologic data from Korean Disease Control and Prevention. Allergy. 2021a;76:921–924. doi: 10.1111/all.14675. - DOI - PMC - PubMed
