

Carotid plaque thickness is increased in chronic kidney disease and associated with carotid and coronary calcification
- PMID: 34813630
- PMCID: PMC8610240
- DOI: 10.1371/journal.pone.0260417
Carotid plaque thickness is increased in chronic kidney disease and associated with carotid and coronary calcification
Abstract
Background: Chronic kidney disease accelerates both atherosclerosis and arterial calcification. The aim of the present study was to explore whether maximal carotid plaque thickness (cPTmax) was increased in patients with chronic kidney disease compared to controls and associated with cardiovascular disease and severity of calcification in the carotid and coronary arteries.
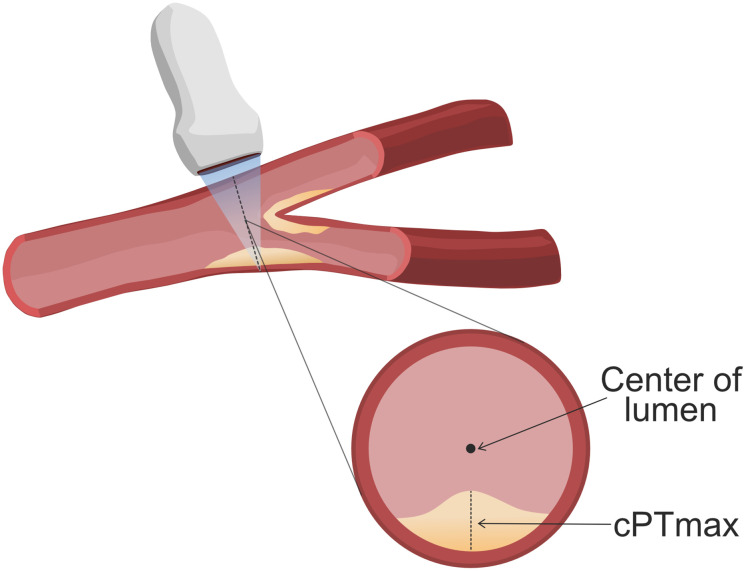
Methods: The study group consisted of 200 patients with chronic kidney disease stage 3 from the Copenhagen Chronic Kidney Disease Cohort and 121 age- and sex-matched controls. cPTmax was assessed by ultrasound and arterial calcification by computed tomography scanning.
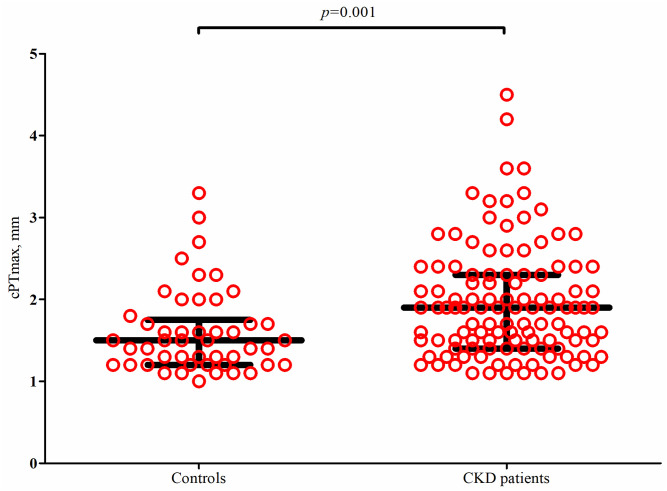
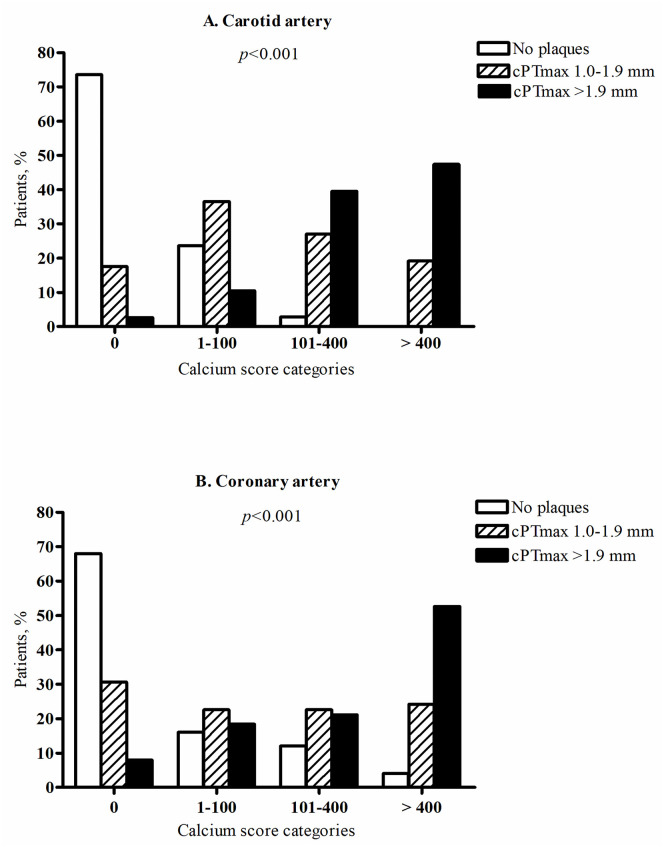
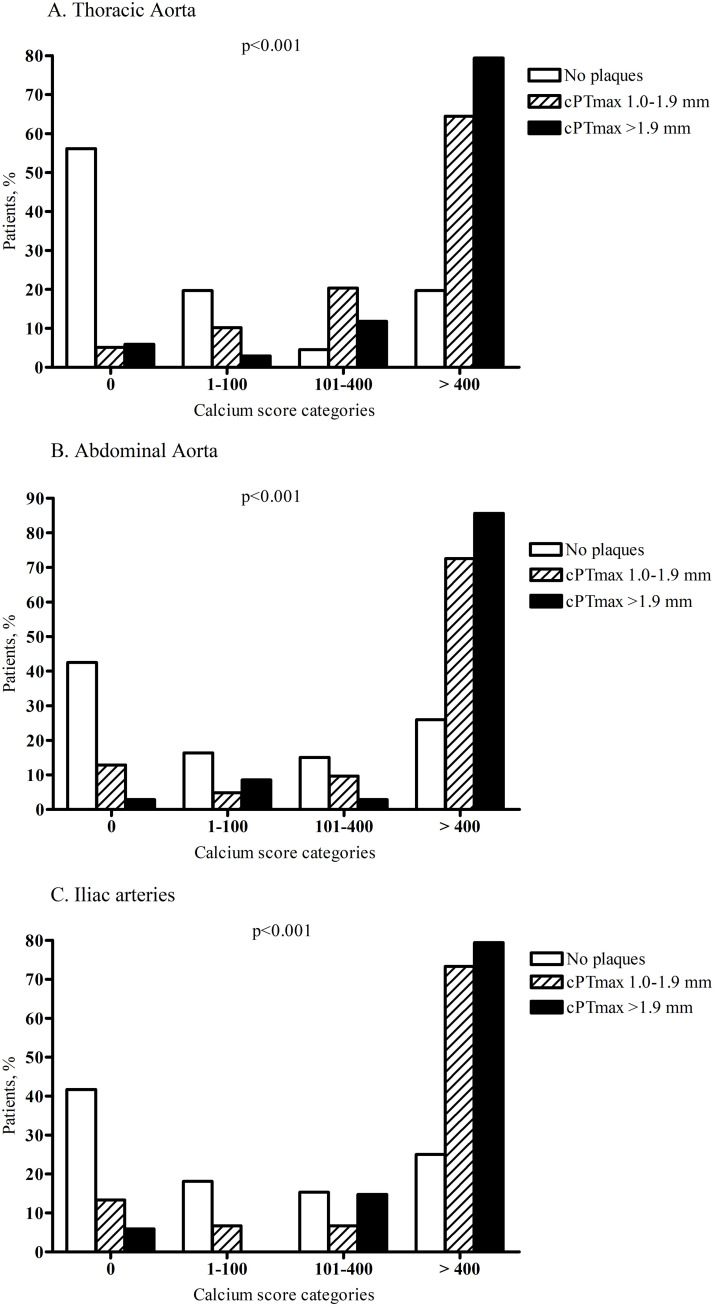
Results: Carotid plaques were present in 58% of patients (n = 115) compared with 40% of controls (n = 48), p = 0.002. Among participants with plaques, cPTmax (median, interquartile range) was significantly higher in patients compared with controls (1.9 (1.4-2.3) versus 1.5 (1.2-1.8) mm), p = 0.001. Cardiovascular disease was present in 9% of patients without plaques (n = 85), 23% of patients with cPTmax 1.0-1.9 mm (n = 69) and 35% of patients with cPTmax >1.9 mm (n = 46), p = 0.001. Carotid and coronary calcium scores >400 were present in 0% and 4%, respectively, of patients with no carotid plaques, in 19% and 24% of patients with cPTmax 1.0-1.9 mm, and in 48% and 53% of patients with cPTmax >1.9 mm, p<0.001.
Conclusions: This is the first study showing that cPTmax is increased in patients with chronic kidney disease stage 3 compared to controls and closely associated with prevalent cardiovascular disease and severity of calcification in both the carotid and coronary arteries.
Conflict of interest statement
I have read the journal´s policy and the authors of this manuscript have the following competing interests: BFR reports research grants from The NovoNordisk Foundation (Steno Collaborative Grant), HS reports research grants from Philips Ultrasound and Bayer and honoraria from Bayer, Novo Nordisk, Bracco and Philips Ultrasound, TBS reports research grants from Sanofi Pasteur and GE Healthcare, the Lundbeck Foundation and the Novo Nordisk Foundation during the conduct of the study. All other authors: no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
