

Characteristics of in-hospital mortality of congenital heart disease (CHD) after surgical treatment in children from 2005 to 2017: a single-center experience
- PMID: 34814864
- PMCID: PMC8609813
- DOI: 10.1186/s12887-021-02935-2
Characteristics of in-hospital mortality of congenital heart disease (CHD) after surgical treatment in children from 2005 to 2017: a single-center experience
Abstract
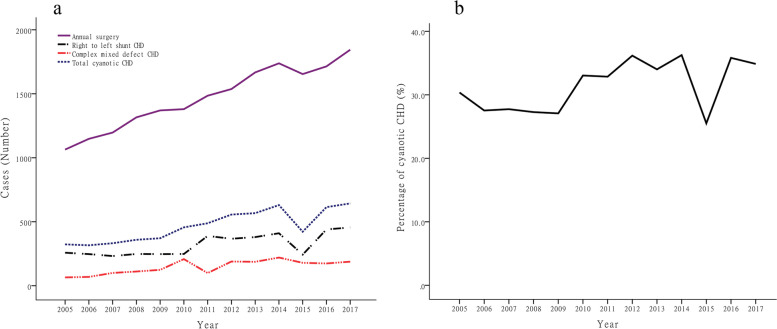
Background: To evaluate trends in the in-hospital mortality rate for pediatric cardiac surgery procedures between 2005 and 2017 in our center, and to discuss the mortality characteristics of children's CHD after thoracotomy.
Methods: This retrospective data were collected from medical records of children underwent CHD surgery between 2005 and 2017.
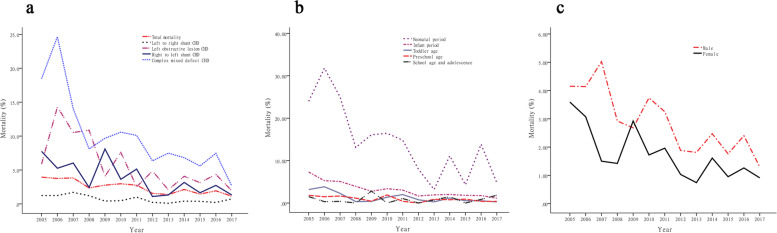
Results: A total of 19,114 children with CHD underwent surgery and 444 children died, with the in-hospital mortality was 2.3%. Complex mixed defect CHD had the highest fatality rate (8.63%), left obstructive lesion CHD had the second highest fatality rate (4.49%), right to left shunt CHD had the third highest mortality rate (3.51%), left to right shunt CHD had the lowest mortality rate (χ2 = 520.3,P < 0.05). The neonatal period has the highest mortality rate (12.17%), followed by infant mortality (2.58%), toddler age mortality (1.16%), and preschool age mortality (0.94%), the school age and adolescent mortality rate was the lowest (χ2 = 529.3,P < 0.05). In addition, the fatality rate in boys was significantly higher than that in girls (2.77% versus 1.62%, χ2 = 26.4, P < 0.05).
Conclusions: The mortality rate of CHD surgery in children decreased year by year. The younger the age and the more complicated the cyanotic heart disease, the higher the mortality rate may be.
Keywords: Congenital heart disease; Epidemiology; In-hospital mortality; Pediatric cardiac surgery.
© 2021. The Author(s).
Conflict of interest statement
All authors stated no potential conflicts exist.
Figures

References
-
- LI Shuo-lin GR-y, Huang G-y. Epidemiological features of congenital heart disease in Chinese children. Chin J Pract Pediatr. 2017;32(11):871–875.
-
- Knowles R, Griebsch I, Dezateux C, Brown J, Bull C, Wren C. Newborn screening for congenital heart defects: a systematic review and cost-effectiveness analysis. Health Technol Assess (Winchester, England) 2005;9(44):1–152. - PubMed
-
- Diller GP, Kempny A, Alonso-Gonzalez R, Swan L, Uebing A, Li W, Babu-Narayan S, Wort SJ, Dimopoulos K, Gatzoulis MA. Survival prospects and circumstances of death in contemporary adult congenital heart disease patients under follow-up at a large tertiary centre. Circulation. 2015;132(22):2118–2125. doi: 10.1161/CIRCULATIONAHA.115.017202. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
