

Immune checkpoint inhibitors plus neoadjuvant chemotherapy in early triple-negative breast cancer: a systematic review and meta-analysis
- PMID: 34814874
- PMCID: PMC8609839
- DOI: 10.1186/s12885-021-08997-w
Immune checkpoint inhibitors plus neoadjuvant chemotherapy in early triple-negative breast cancer: a systematic review and meta-analysis
Abstract
Purpose: Some studies have shown that Immune checkpoint inhibitors (ICIs) have a favorable efficacy in advanced triple negative breast cancer (TNBC) patients, but the results are controversial in neoadjuvant chemotherapy (NACT) stage. The purpose of this study is to evaluate the efficacy and safety after NACT plus ICIs in early TNBC patients.
Methods: After searching PubMed, EMBASE, the Cochrane library and several mainly oncology conferences up to 30 January 2021 systematically, and define randomized controlled trials (RCTs) exploring the efficacy and safety of programmed death protein-1/programmed cell death-Ligand 1(PD-1/PD-L1) inhibitors plus neoadjuvant chemotherapy in TNBC patients. The primary endpoint was the pathological complete response (pCR) in intention-to-treat populations (ITT), and the secondary endpoints were event-free survival (EFS) and safety analysis in the ITT populations.
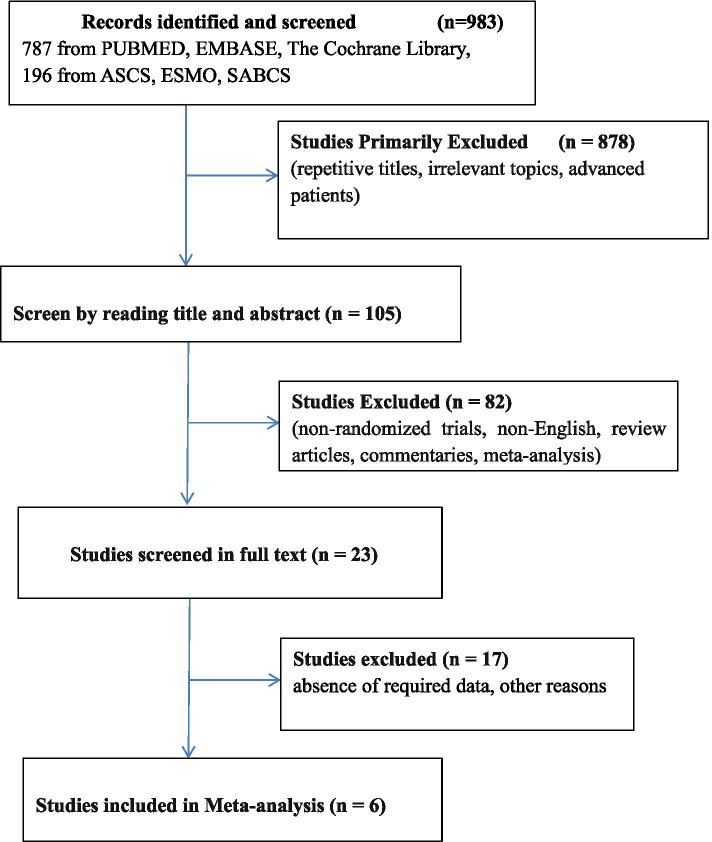
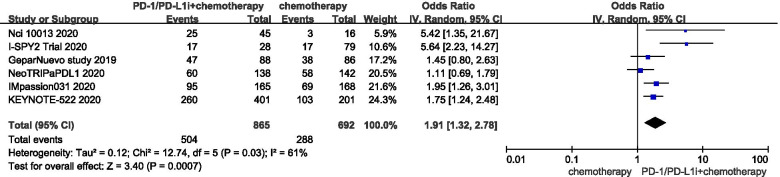
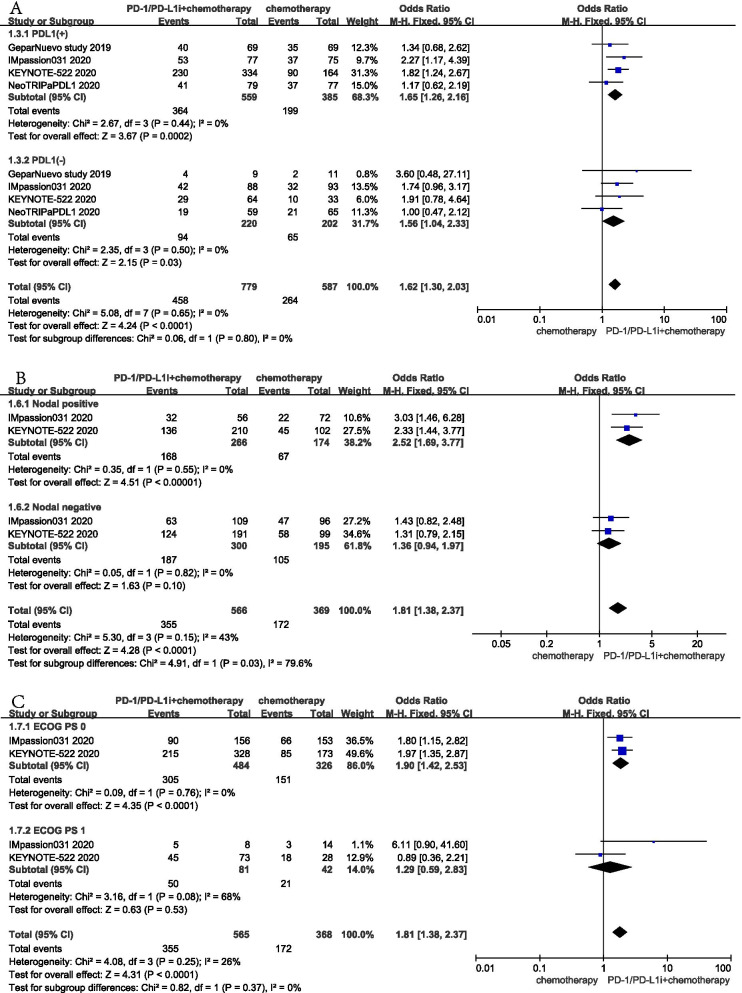
Results: Six RCTs (N = 2142) were included in our meta-analysis; NACT plus ICIs increased pCR rates compared with NACT in intention-to-treat (ITT) populations (OR: 1.91; 95% CI: 1.32-2.78, P < 0.001). The pCR rate also increased in both PD-L1 positive (OR: 1.65; 95% CI: 1.26-2.16, P < 0.001) and PD-L1 negative patients (OR: 1.56; 95% CI: 1.04-2.33, P = 0.03), especially in PD-L1 positive patients. The benefit was also observed in nodal-positive populations (OR: 2.52; 95% CI: 1.69-3.77, P < 0.001) and Eastern Cooperative Oncology Group performance-status score (ECOG PS) 0 subgroup (OR: 1.90; 95% CI: 1.42-2.53, P < 0.001). Three RCTs (N = 1615) reported EFS and the results showed that adding PD-1/PD-L1 inhibitors increased EFS (HR 0.65, 95% CI 0.50-0.83, P = 0.0007) in ITT populations with a short follow-up time. In the safety analysis of 2205 patients with early TNBC from five eligible studies, NACT plus ICIs had a higher risk of grade 3-4 diarrhea (OR: 2.54; 95% CI: 1.21-5.32; P = 0.01), any grade of adverse effects(AEs)including vomiting (OR: 1.37; 95% CI: 1.00-1.86; P = 0.05), hyperthyroidism (OR: 6.04; 95% CI: 2.39-15.29; P < 0.001), and hypothyroidism (OR: 5.04; 95% CI: 3.02-8.39; P < 0.001).
Conclusions: PD-1/PD-L1 inhibitors combined with chemotherapy can improve pCR rates and EFS, and with an increased incidence of some immune-related AEs compared with chemotherapy alone. NACT plus ICIs might be an option in patients with in PD-L1 positive and high-risk populations with positive nodal disease early TNBC.
Keywords: Neoadjuvant chemotherapy; PD-1/PD-L1 inhibitors; Triple-negative breast cancer.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests
Figures

References
-
- Bergin ART, Loi S. Triple-negative breast cancer: recent treatment advances. F1000Res. 2019;8:F1000 Faculty Rev-1342. 10.12688/f1000research.18888.1. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
