

Promises and challenges of personalized medicine to guide ARDS therapy
- PMID: 34814925
- PMCID: PMC8609268
- DOI: 10.1186/s13054-021-03822-z
Promises and challenges of personalized medicine to guide ARDS therapy
Abstract
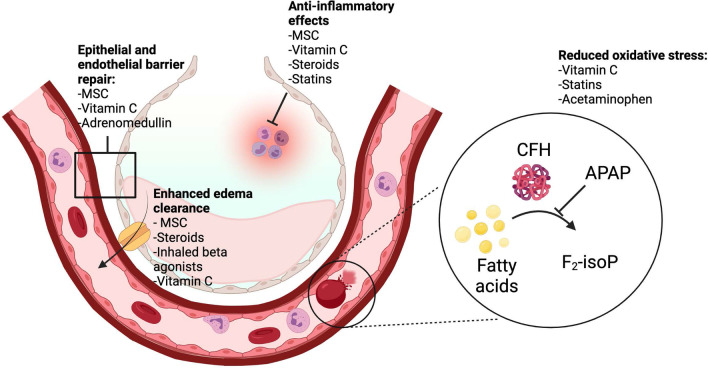
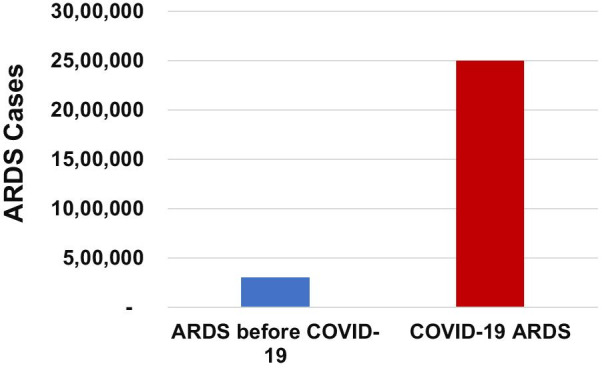
Identifying new effective treatments for the acute respiratory distress syndrome (ARDS), including COVID-19 ARDS, remains a challenge. The field of ARDS investigation is moving increasingly toward innovative approaches such as the personalization of therapy to biological and clinical sub-phenotypes. Additionally, there is growing recognition of the importance of the global context to identify effective ARDS treatments. This review highlights emerging opportunities and continued challenges for personalizing therapy for ARDS, from identifying treatable traits to innovative clinical trial design and recognition of patient-level factors as the field of critical care investigation moves forward into the twenty-first century.
Keywords: Acute lung injury; Acute respiratory distress syndrome; COVID-19; Clinical trials; Personalized medicine.
© 2021. The Author(s).
Conflict of interest statement
KDW has received funding from NIH 5T32GM8440-24. DFM: Funding for PHIND trial from Innovate UK; grants/contracts from NIHR, Wellcome Trust, MRC, Northern Ireland HSC R&D division, and Novavax as an investigator for ARDS and Covid-19 trials; patent from Queen’s Belfast University for novel treatment for inflammatory disease (USB962032); consulting fees from Bayer, GlaxoSmithKline, Boehringer Ingelheim, Novartis, and Eli Lilly for the study of ARDS and Covid-19; Speaker fees from GlaxoSmithKline for educational seminars; DSMB member for Vir Biotechnology, Inc. and Faron Pharmaceuticals; Co-director of research for the Intensive Care Society; Director of EME program for MRC/NIHR. Spouse has received consultancy fees from Insmed and the California Institute for Regenerative medicine. JEL has received a grant from the NIH (UH3HL141722) to study inhaled budesonide and formoterol for the treatment of hospitalized patients with pneumonia and hypoxemia for the prevention of acute respiratory failure. JRB: Grant funding from NIH grants K23-HL133489 and R21-HL145506. Consulting fees from Sedana Medical and Biomarck Pharmaceuticals for clinical trial design/planning, and Hamilton Medical for work as a medical monitor. DA has received a public grant through the national program “Programme d’Investissements d’avenir” under the reference ANR-18-RHUS-0004 for investigating corticosteroid therapy in COVID-19 and sepsis. This work is part of Federations Hospitalo-universitaires (FHU) Saclay and Paris Seine Nord Endeavour to PerSonalize Interventions for Sepsis (SEPSIS). EDR declares no competing interests. CSC: Grant funding from the NIH for the investigation of ARDS; grant support from Roche/Genentech, and Bayer for observational studies of ARDS; consultancy fees from Roche/Genentech, Bayer, Gen1e Life Sciences, and Vasomune; fees for serving on the medical board of Prometric and Quark Pharmaceuticals; personal fees from Quantum Leap Healthcare Collaborative. MAM: Grant funding from the NIH for the investigation of ARDS; grant support from Roche/Genentech for observational studies of ARDS; consulting income from Citius Pharmaceuticals, Johnson and Johnson, and Novartis.
Figures

References
-
- Sinha P, Delucchi KL, Chen Y, Zhuo H, Abbott J, Wang C, Wickersham N, McNeil JB, Jauregui A, Ke S, Vessel K, Gomez A, Hendrickson CM, Kangelaris KN, Sarma A, Leligdowicz A, Liu KD, Matthay MA, Ware LB, Calfee CS. Latent class analysis-derived subphenotypes are generalisable to observational cohorts of acute respiratory distress syndrome: a prospective study. Thorax. 2021. 10.1136/thoraxjnl-2021-217158. - PMC - PubMed
-
- Calfee CS, Delucchi KL, Sinha P, Matthay MA, Hackett J, Shankar-Hari M, McDowell C, Laffey JG, O'Kane CM, McAuley DF, et al. Acute respiratory distress syndrome subphenotypes and differential response to simvastatin: secondary analysis of a randomised controlled trial. Lancet Respir Med. 2018;6(9):691–698. - PMC - PubMed
