

Assessment of histological characteristics, imaging markers, and rt-PA susceptibility of ex vivo venous thrombi
- PMID: 34815441
- PMCID: PMC8610976
- DOI: 10.1038/s41598-021-02030-7
Assessment of histological characteristics, imaging markers, and rt-PA susceptibility of ex vivo venous thrombi
Abstract
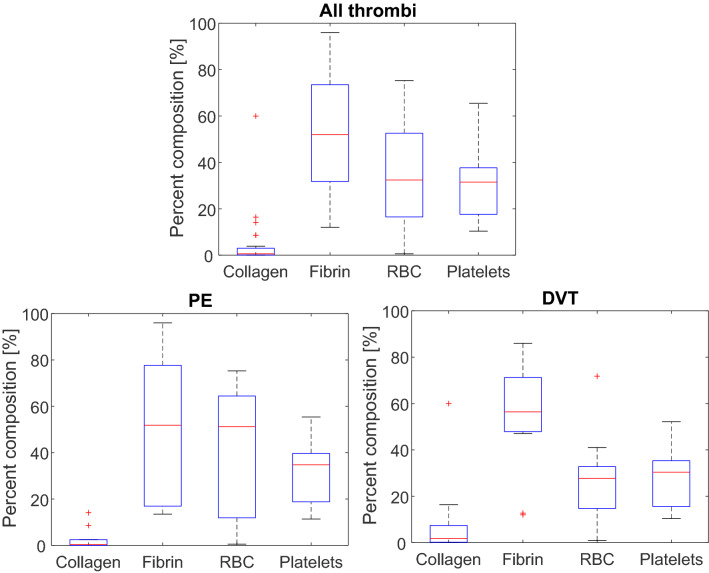
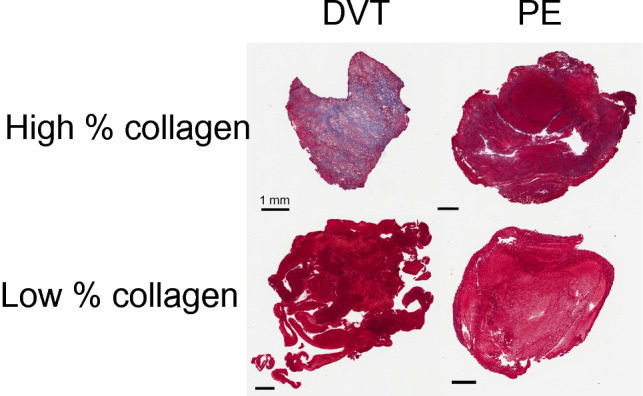
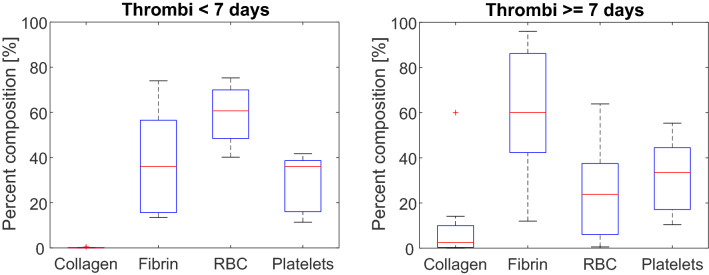
Venous thromboembolism is a significant source of morbidity and mortality worldwide. Catheter-directed thrombolytics is the primary treatment used to relieve critical obstructions, though its efficacy varies based on the thrombus composition. Non-responsive portions of the specimen often remain in situ, which prohibits mechanistic investigation of lytic resistance or the development of diagnostic indicators for treatment outcomes. In this study, thrombus samples extracted from venous thromboembolism patients were analyzed ex vivo to determine their histological properties, susceptibility to lytic therapy, and imaging characteristics. A wide range of thrombus morphologies were observed, with a dependence on age and etymology of the specimen. Fibrinolytic inhibitors including PAI-1, alpha 2-antiplasmin, and TAFI were present in samples, which may contribute to the response venous thrombi to catheter-directed thrombolytics. Finally, a weak but significant correlation was observed between the response of the sample to lytic drug and its magnetic microstructure assessed with a quantitative MRI sequence. These findings highlight the myriad of changes in venous thrombi that may promote lytic resistance, and imaging metrics that correlate with treatment outcomes.
© 2021. The Author(s).
Conflict of interest statement
K.B.B. obtains funding from the National Institutes of Health (Grant Number R01 HL133334). O. A. has acted as a consultant for Inari Medical, Boston Scientific, and received research grants from Inari Medical, Canon Medical, and Philips. He acted as a speaker and received compensation for Argon Medical, Canon Medical, Penumbra, Philips, and Johnson and Johnson. G.D.W. received honoraria and serves on the advisory board for Diagnostica Stago. S.A.H., A.B., A.D., E.S., D.M., R.O.A., Y.Z., S.S., Z.F.L., J.D.P. declare no potential conflict of interest.
Figures




References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
