

Nutcracker syndrome: diagnosis and therapy
- PMID: 34815965
- PMCID: PMC8569268
- DOI: 10.21037/cdt-20-160
Nutcracker syndrome: diagnosis and therapy
Abstract
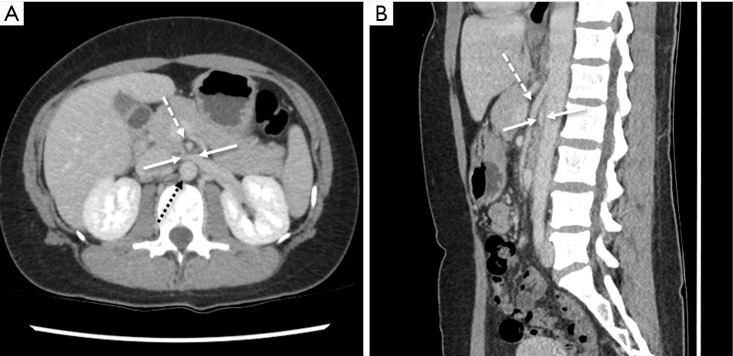
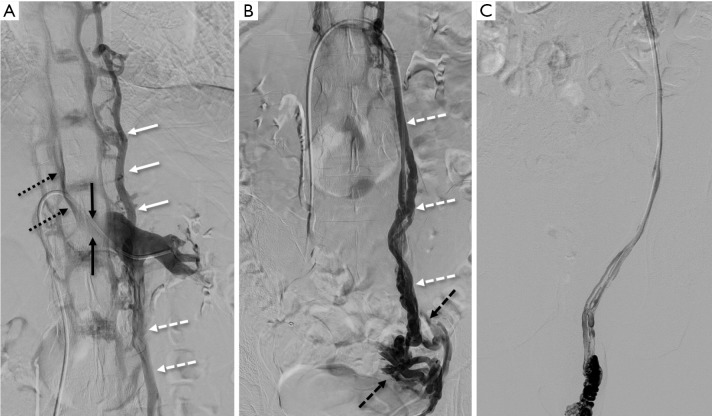
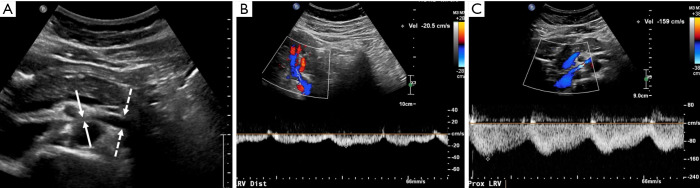
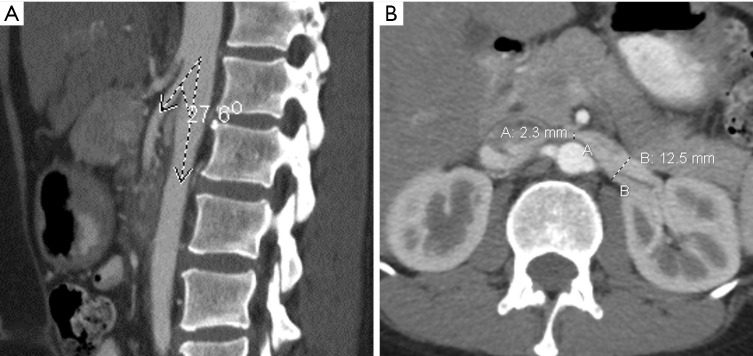
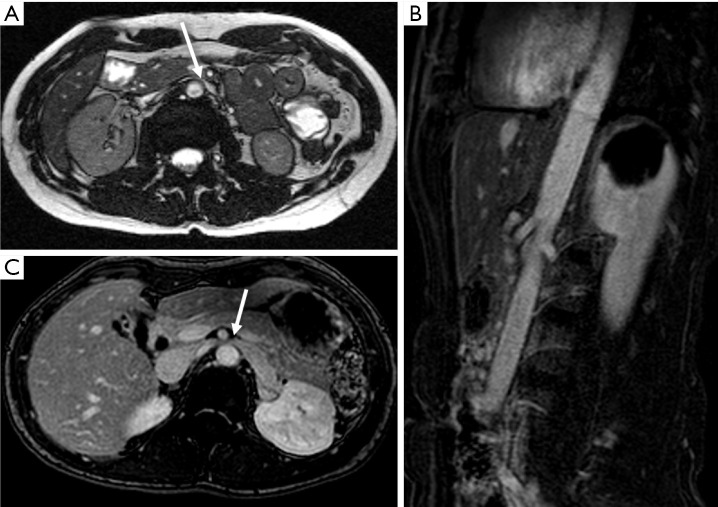
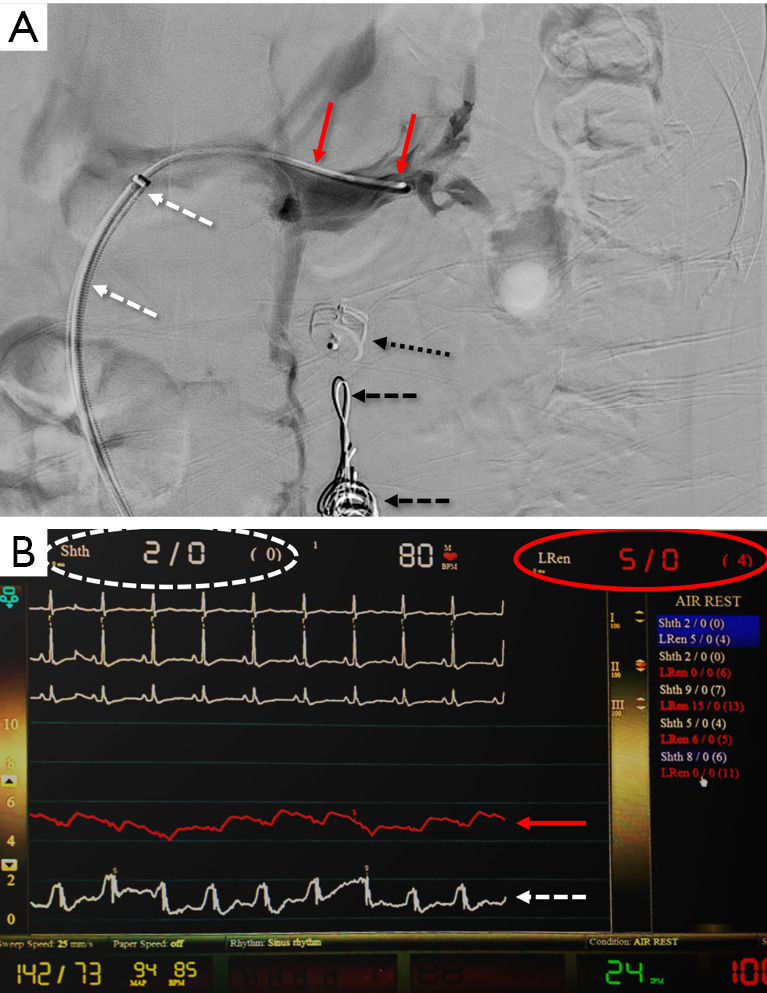
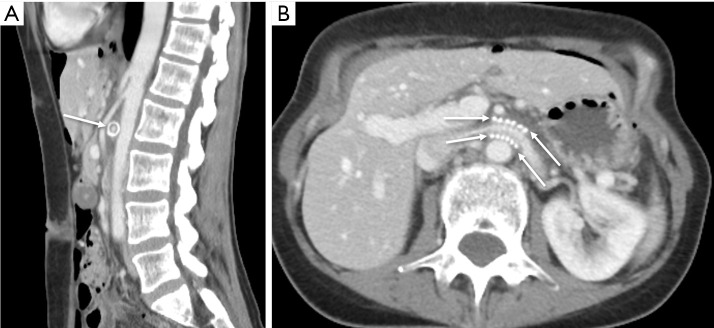
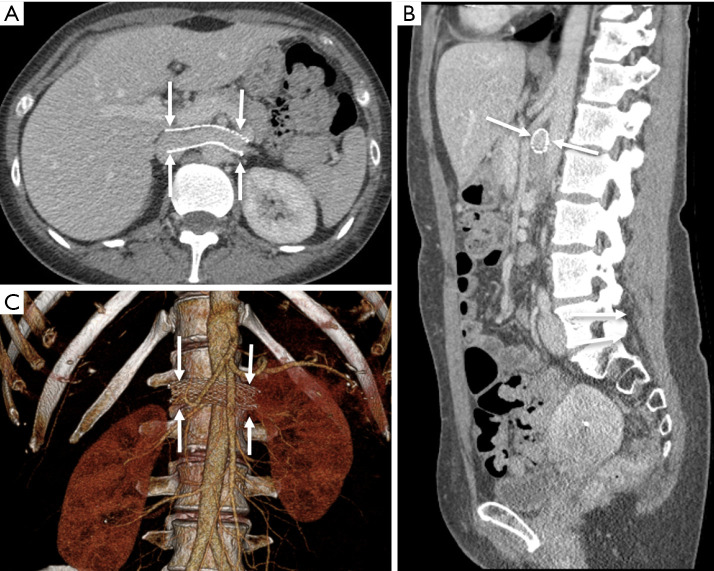
Nutcracker syndrome (NCS) is an extrinsic compression of the left renal vein (LRV) by the superior mesenteric artery (SMA) anteriorly and aorta posteriorly resulting in renal vascular congestion manifesting as hematuria, proteinuria, orthostatic hypotension, pain, or even renal dysfunction. Long-standing venous compression can encourage collateral drainage pathways through gonadal and pelvic veins, which may explain reported symptom and syndrome overlap with pelvic congestion syndrome. Diagnosis can be challenging and variable, frequently involving a combination of ultrasound Doppler, cross-sectional, and invasive imaging. Often, intravascular pressure measurements are required to prove a renocaval pressure gradient to aid in a definitive diagnosis. Conservative management is appropriate, especially in children, who tend to outgrow the disorder. In the interim, medical management with angiotensin converting enzyme inhibitors (ACEIs) is a useful therapy to manage orthostatic hypotension in the pediatric population. In adults, invasive therapies are more frequently pursued. These are aimed at relieving the extrinsic compression on the LRV. The standard of care is renal vein transposition, with renal autotransplantation reserved for recalcitrant cases. Endovascular stenting is a less invasive option. Laparoscopic placement of an exovascular stent is a newer therapy intended to minimize trauma to the LRV. In this review, we will discuss the clinical manifestations, diagnostic criterion, imaging features, and conservative and surgical therapies for this condition.
Keywords: Nutcracker syndrome (NCS); hematuria; left renal vein (LRV); vascular compression.
2021 Cardiovascular Diagnosis and Therapy. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/cdt-20-160). The series “Compressive Vascular Syndromes” was commissioned by the editorial office without any funding or sponsorship. Drs. MKK and SK served as the unpaid Guest Editors of the series. Dr. SK serves as an unpaid editorial board member of Cardiovascular Diagnosis and Therapy from May 2019 to Apr 2021. Dr. SK reports personal fees from Medtronic, personal fees from Dova Pharmaceuticals, personal fees from Koo Foundation, Taiwan, personal fees from GE healthcare, personal fees from Springer, personal fees from Elsevier, other from Althea Health Inc, CA, personal fees from Boston Scientific, personal fees from Penumbra, grants from BD, grants from NIH, outside the submitted work. The authors have no other conflicts of interest to declare.
Figures

References
-
- de Schepper A. "Nutcracker" phenomenon of the renal vein and venous pathology of the left kidney. J Belge Radiol 1972;55:507-11. - PubMed
Publication types
LinkOut - more resources
Full Text Sources