

Global prevalence of sarcopenia and severe sarcopenia: a systematic review and meta-analysis
- PMID: 34816624
- PMCID: PMC8818604
- DOI: 10.1002/jcsm.12783
Global prevalence of sarcopenia and severe sarcopenia: a systematic review and meta-analysis
Abstract
Background: Sarcopenia is defined as the loss of muscle mass and strength. Despite the seriousness of this disease, a single diagnostic criterion has not yet been established. Few studies have reported the prevalence of sarcopenia globally, and there is a high level of heterogeneity between studies, stemmed from the diagnostic criteria of sarcopenia and the target population. The aims of this systematic review and meta-analysis were (i) to identify and summarize the diagnostic criteria used to define sarcopenia and severe sarcopenia and (ii) to estimate the global and region-specific prevalence of sarcopenia and severe sarcopenia by sociodemographic factors.
Methods: Embase, MEDLINE, and Web of Science Core Collections were searched using relevant MeSH terms. The inclusion criteria were cross-sectional or cohort studies in individuals aged ≥18 years, published in English, and with muscle mass measured using dual-energy x-ray absorptiometry, bioelectrical impedance, or computed tomography (CT) scan. For the meta-analysis, studies were stratified by diagnostic criteria (classifications), cut-off points, and instruments to assess muscle mass. If at least three studies reported the same classification, cut-off points, and instrument to measure muscle mass, they were considered suitable for meta-analysis. Following this approach, 6 classifications and 23 subgroups were created. Overall pooled estimates with inverse-variance weights obtained from a random-effects model were estimated using the metaprop command in Stata.
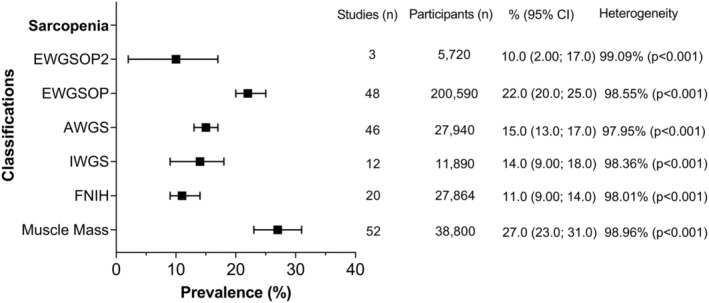
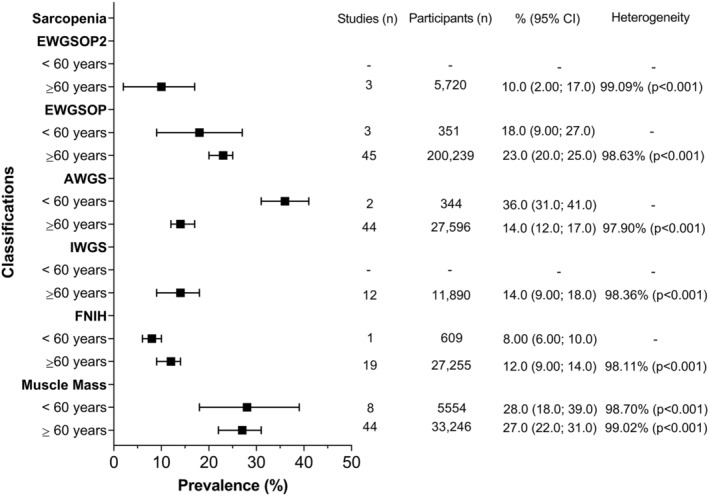
Results: Out of 19 320 studies, 263 were eligible for the narrative synthesis and 151 for meta-analysis (total n = 692 056, mean age: 68.5 years). Using different classifications and cut-off points, the prevalence of sarcopenia varied between 10% and 27% in the studies included for meta-analysis. The highest and lowest prevalence were observed in Oceania and Europe using the European Working Group on Sarcopenia in Older People (EWGSOP) and EWGSOP2, respectively. The prevalence ranged from 8% to 36% in individuals <60 years and from 10% to 27% in ≥60 years. Men had a higher prevalence of sarcopenia using the EWGSOP2 (11% vs. 2%) while it was higher in women using the International Working Group on Sarcopenia (17% vs. 12%). Finally, the prevalence of severe sarcopenia ranged from 2% to 9%.
Conclusions: The prevalence of sarcopenia and severe sarcopenia varied considerably according to the classification and cut-off point used. Considering the lack of a single diagnostic for sarcopenia, future studies should adhere to current guidelines, which would facilitate the comparison of results between studies and populations across the globe.
Keywords: Meta-analysis; Prevalence; Sarcopenia; Systematic review.
© 2021 The Authors. Journal of Cachexia, Sarcopenia and Muscle published by John Wiley & Sons Ltd on behalf of Society on Sarcopenia, Cachexia and Wasting Disorders.
Conflict of interest statement
None to declare.
Figures





References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
