

Machine learning optimization of an electronic health record audit for heart failure in primary care
- PMID: 34816632
- PMCID: PMC8787980
- DOI: 10.1002/ehf2.13724
Machine learning optimization of an electronic health record audit for heart failure in primary care
Abstract
Aims: The diagnosis of heart failure (HF) is an important problem in primary care. We previously demonstrated a 74% increase in registered HF diagnoses in primary care electronic health records (EHRs) following an extended audit procedure. What remains unclear is the accuracy of registered HF pre-audit and which EHR variables are most important in the extended audit strategy. This study aims to describe the diagnostic HF classification sequence at different stages, assess general practitioner (GP) HF misclassification, and test the predictive performance of an optimized audit.
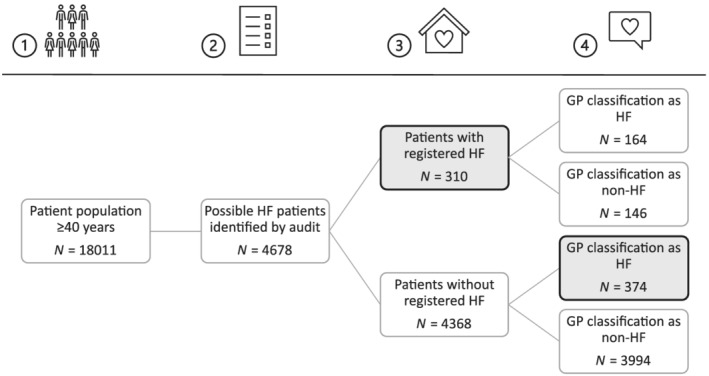
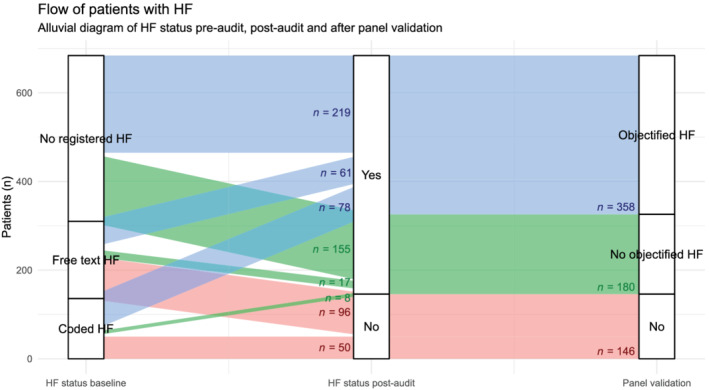
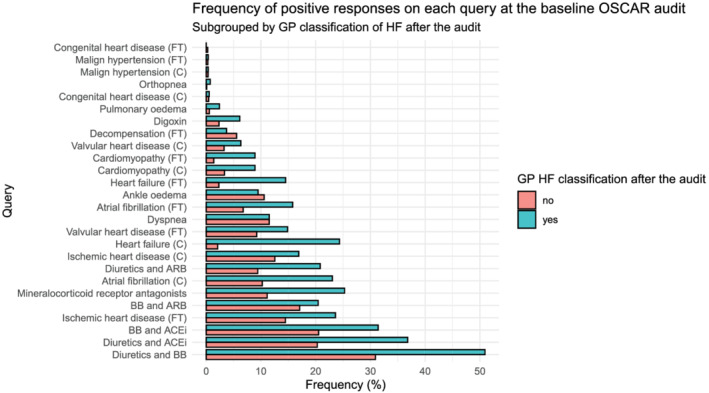
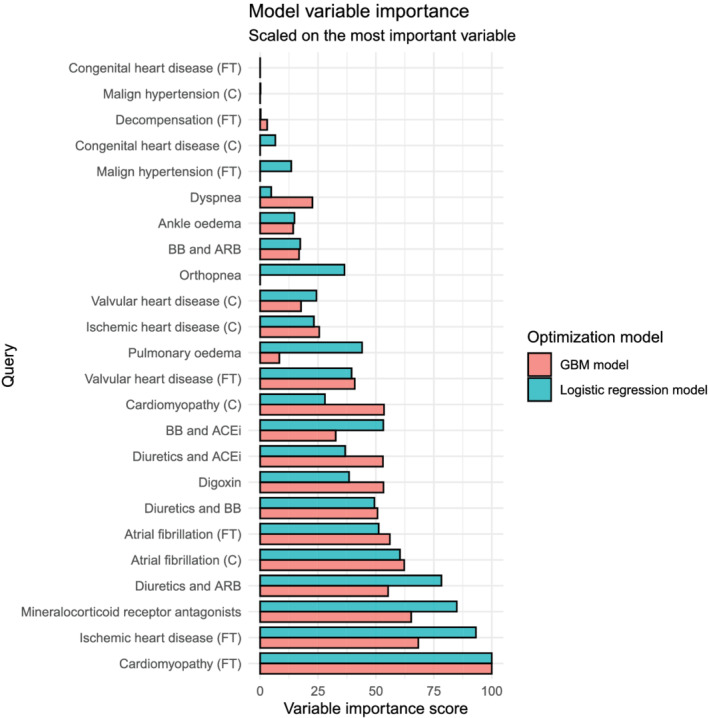
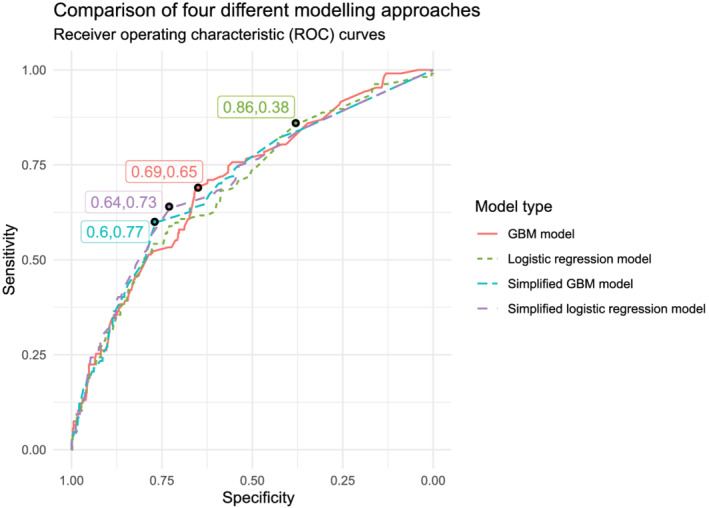
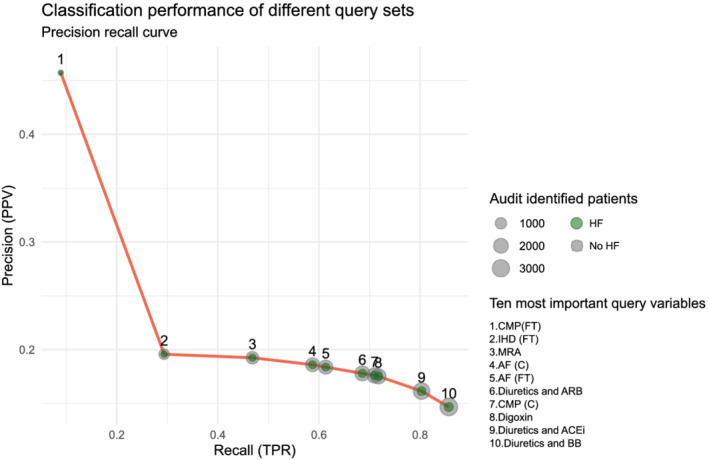
Methods and results: This is a secondary analysis of the OSCAR-HF study, a prospective observational trial including 51 participating GPs. OSCAR used an extended audit based on typical HF risk factors, signs, symptoms, and medications in GPs' EHR. This resulted in a list of possible HF patients, which participating GPs had to classify as HF or non-HF. We compared registered HF diagnoses before and after GPs' assessment. For our analysis of audit performance, we used GPs' assessment of HF as primary outcome and audit queries as dichotomous predictor variables for a gradient boosted machine (GBM) decision tree algorithm and logistic regression model. Of the 18 011 patients eligible for the audit intervention, 4678 (26.0%) were identified as possible HF patients and submitted for GPs' assessment in the audit stage. There were 310 patients with registered HF before GP assessment, of whom 146 (47.1%) were judged not to have HF by their GP (over-registration). There were 538 patients with registered HF after GP assessment, of whom 374 (69.5%) did not have registered HF before GP assessment (under-registration). The GBM and logistic regression model had a comparable predictive performance (area under the curve of 0.70 [95% confidence interval 0.65-0.77] and 0.69 [95% confidence interval 0.64-0.75], respectively). This was not significantly impacted by reducing the set of predictor variables to the 10 most important variables identified in the GBM model (free-text and coded cardiomyopathy, ischaemic heart disease and atrial fibrillation, digoxin, mineralocorticoid receptor antagonists, and combinations of renin-angiotensin system inhibitors and beta-blockers with diuretics). This optimized query set was enough to identify 86% (n = 461/538) of GPs' self-assessed HF population with a 33% reduction (n = 1537/4678) in screening caseload.
Conclusions: Diagnostic coding of HF in primary care health records is inaccurate with a high degree of under-registration and over-registration. An optimized query set enabled identification of more than 80% of GPs' self-assessed HF population.
Keywords: Audit and feedback; Chronic heart failure; Electronic health records; Primary care; Screening.
© 2021 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
W.R., M.S., S.H., B.A., J.P., W.M., and B.V. report no conflict of interest. S.J. is holder of a named chair in Cardiology at the University of Leuven financed by Astra‐Zeneca.
Figures
Similar articles
-
Mixed-methods evaluation of a multifaceted heart failure intervention in general practice: the OSCAR-HF pilot study.ESC Heart Fail. 2023 Apr;10(2):907-916. doi: 10.1002/ehf2.14251. Epub 2022 Dec 3. ESC Heart Fail. 2023. PMID: 36461750 Free PMC article.
-
Impact of an extended audit on identifying heart failure patients in general practice: baseline results of the OSCAR-HF pilot study.ESC Heart Fail. 2020 Dec;7(6):3950-3961. doi: 10.1002/ehf2.12990. Epub 2020 Sep 24. ESC Heart Fail. 2020. PMID: 32969599 Free PMC article.
-
Factors associated with general practitioners' awareness of depression in primary care patients with heart failure: baseline-results from the observational RECODE-HF study.BMC Fam Pract. 2017 Jun 9;18(1):71. doi: 10.1186/s12875-017-0641-1. BMC Fam Pract. 2017. PMID: 28599626 Free PMC article.
-
Optimising standards of care of heart failure in general practice the OSCAR-HF pilot study protocol.Acta Cardiol. 2019 Oct;74(5):371-379. doi: 10.1080/00015385.2018.1507426. Epub 2018 Dec 3. Acta Cardiol. 2019. PMID: 30507291
-
Machine learning: at the heart of failure diagnosis.Curr Opin Cardiol. 2021 Mar 1;36(2):227-233. doi: 10.1097/HCO.0000000000000833. Curr Opin Cardiol. 2021. PMID: 33443957 Review.
Cited by
-
AI driven mechanical circulatory support: Can AI and Impella team up to beat cardiogenic shock.ESC Heart Fail. 2024 Oct;11(5):2487-2489. doi: 10.1002/ehf2.14995. Epub 2024 Jul 24. ESC Heart Fail. 2024. PMID: 39049432 Free PMC article. No abstract available.
-
Mixed-methods evaluation of a multifaceted heart failure intervention in general practice: the OSCAR-HF pilot study.ESC Heart Fail. 2023 Apr;10(2):907-916. doi: 10.1002/ehf2.14251. Epub 2022 Dec 3. ESC Heart Fail. 2023. PMID: 36461750 Free PMC article.
-
How to Evaluate Online Education for General Practitioners: Development of a Tailored Questionnaire for Heart Failure Education.J Med Educ Curric Dev. 2024 Mar 9;11:23821205241232497. doi: 10.1177/23821205241232497. eCollection 2024 Jan-Dec. J Med Educ Curric Dev. 2024. PMID: 38464745 Free PMC article.
References
-
- Groenewegen A, Rutten FH. Near‐home heart failure care. Eur J Heart Fail 2019; 21: 110–111. - PubMed
-
- van Riet EE, Hoes AW, Limburg A, Landman MA, van der Hoeven H, Rutten FH. Prevalence of unrecognized heart failure in older persons with shortness of breath on exertion. Eur J Heart Fail 2014; 16: 772–777. - PubMed
-
- Dahlstrom U, Hakansson J, Swedberg K, Waldenstrom A. Adequacy of diagnosis and treatment of chronic heart failure in primary health care in Sweden. Eur J Heart Fail 2009; 11: 92–98. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
