

Fecal microbiome and bile acid metabolome in adult short bowel syndrome
- PMID: 34816756
- PMCID: PMC8793869
- DOI: 10.1152/ajpgi.00091.2021
Fecal microbiome and bile acid metabolome in adult short bowel syndrome
Abstract
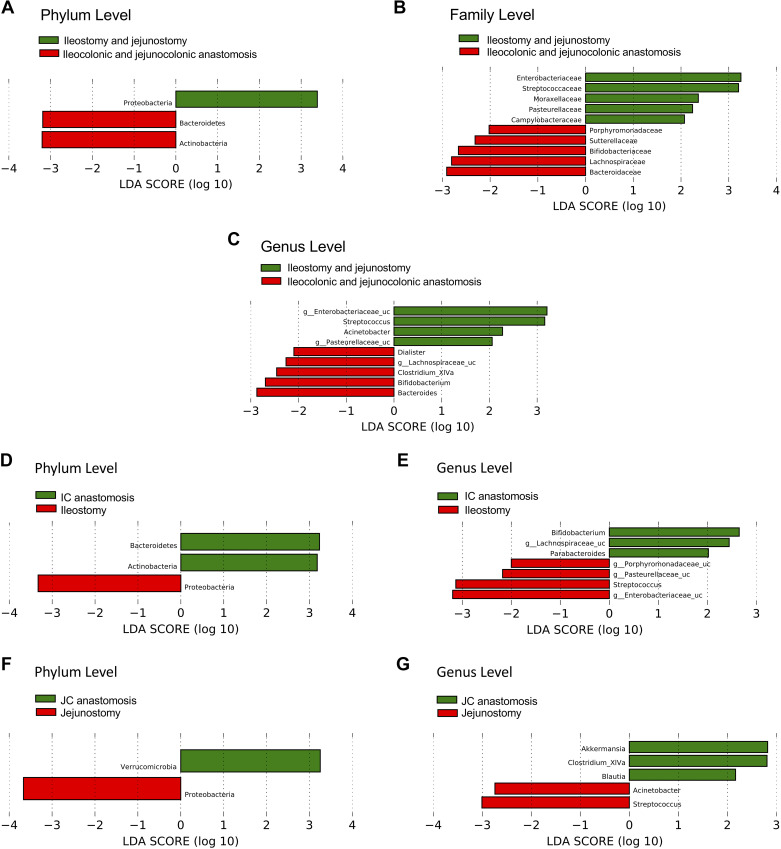
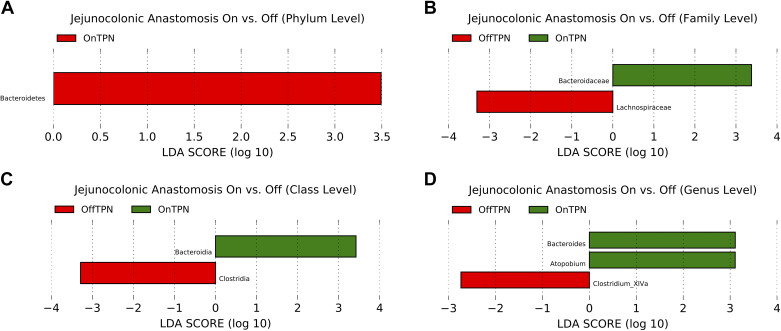
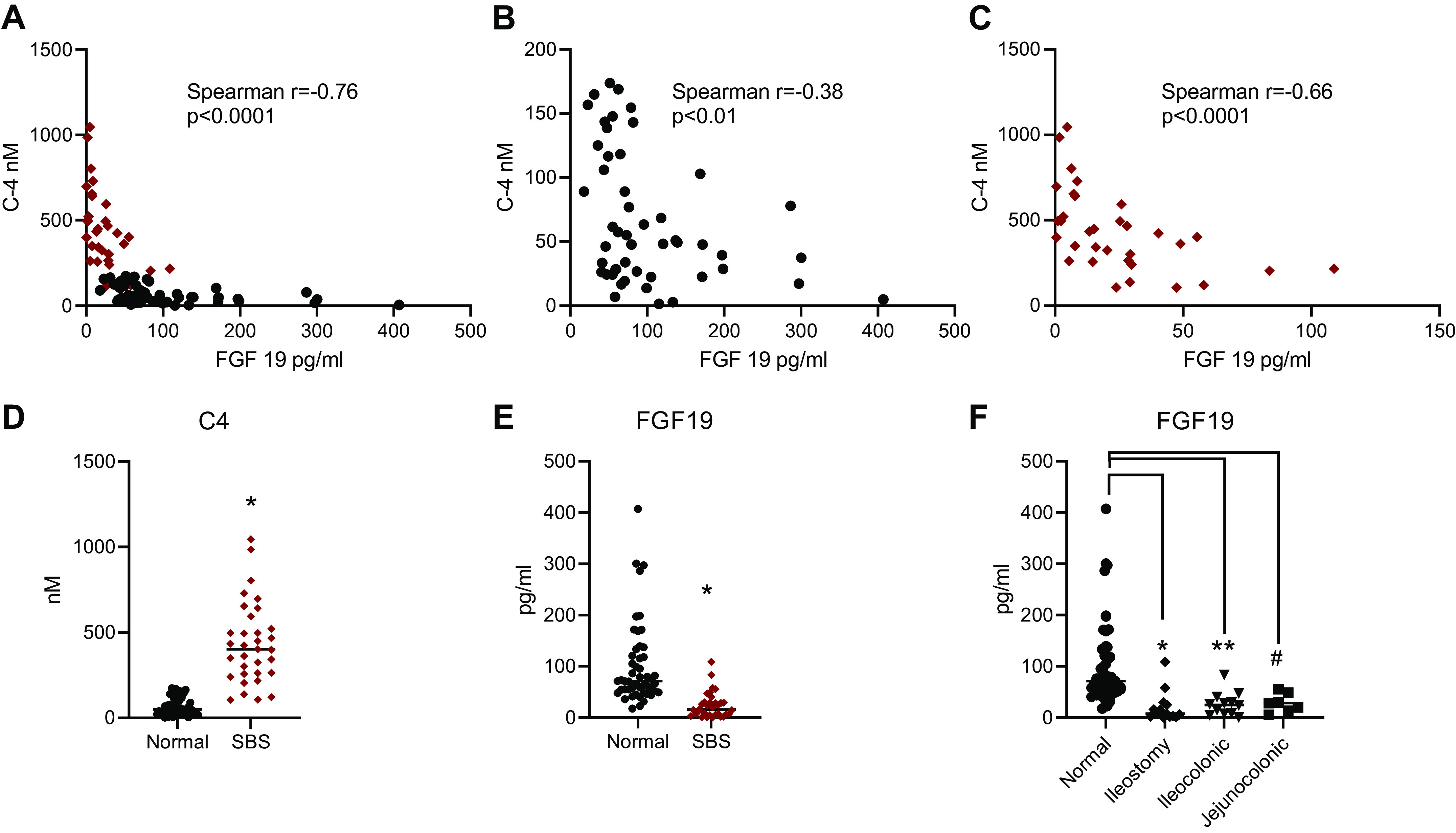
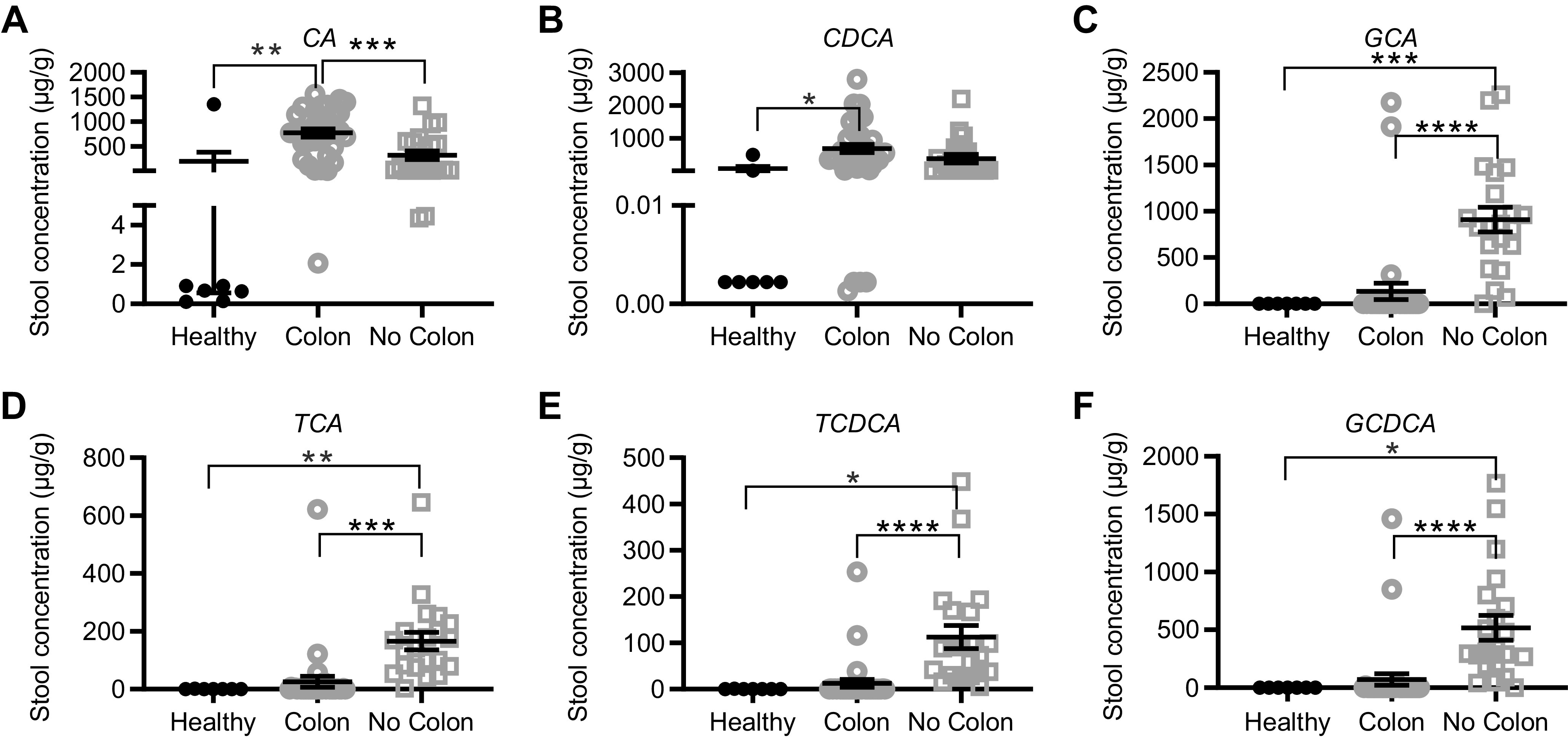
Loss of functional small bowel surface area causes short bowel syndrome (SBS), intestinal failure, and parenteral nutrition (PN) dependence. The gut adaptive response following resection may be difficult to predict, and it may take up to 2 yr to determine which patients will wean from PN. Here, we examined features of gut microbiota and bile acid (BA) metabolism in determining adaptation and ability to wean from PN. Stool and sera were collected from healthy controls and from patients with SBS (n = 52) with ileostomy, jejunostomy, ileocolonic, and jejunocolonic anastomoses fed with PN plus enteral nutrition or who were exclusively enterally fed. We undertook 16S rRNA gene sequencing, BA profiling, and 7α-hydroxy-4-cholesten-3-one (C4) quantitation with LC-MS/MS and serum amino acid analyses. Patients with SBS exhibited altered gut microbiota with reduced gut microbial diversity compared with healthy controls. We observed differences in the microbiomes of patients with SBS with ileostomy versus jejunostomy, jejunocolonic versus ileocolonic anastomoses, and PN dependence compared with those who weaned from PN. Stool and serum BA composition and C4 concentrations were also altered in patients with SBS, reflecting adaptive changes in enterohepatic BA cycling. Stools from patients who were weaned from PN were enriched in secondary BAs including deoxycholic acid and lithocholic aicd. Shifts in gut microbiota and BA metabolites may generate a favorable luminal environment in select patients with SBS, promoting the ability to wean from PN. Proadaptive microbial species and select BA may provide novel targets for patient-specific therapies for SBS.NEW & NOTEWORTHY Loss of intestinal surface area causes short bowel syndrome, intestinal failure, and parenteral nutrition dependence. We analyzed the gut microbiota and bile acid metabolome of a large cohort of short bowel syndrome adult patients with different postsurgical anatomies. We report a novel analysis of the microbiome of patients with ileostomy and jejunostomy. Enrichment of specific microbial and bile acid species may be associated with the ability to wean from parenteral nutrition.
Keywords: FGF19; enterohepatic bile acid cycling; intestinal adaptation; short gut syndrome.
Conflict of interest statement
P. Tarr has an equity interest in, and is a member of the Scientific Advisory Board of, and a consultant to, MediBeacon Inc., which is developing a noninvasive technique to measure intestinal permeability in humans. P. Tarr is also a coinventor on a patent related to this technology, which might generate royalty payments. None of the other authors has any conflicts of interest, financial or otherwise, to disclose. Writing of this paper and data analysis were not funded by additional organizations, and there was no writing support provided by any additional individuals, organizations, or companies.
Figures







References
-
- Levin MS, Rubin DC. Intestinal adaptation: the biology of the intestinal response to resection and disease. In: Intestinal Failure: Diagnosis Management and Transplantation, edited by Langnas AN, Quigley EMM, Tappenden KA.. Malden, MA: Blackwell Publishing, 2008, p. 45–54.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous