

Rapid Diagnostic Tests to Guide Case Management of and Improve Antibiotic Stewardship for Pediatric Acute Respiratory Illnesses in Resource-Constrained Settings: a Prospective Cohort Study in Southwestern Uganda
- PMID: 34817224
- PMCID: PMC8612158
- DOI: 10.1128/Spectrum.01694-21
Rapid Diagnostic Tests to Guide Case Management of and Improve Antibiotic Stewardship for Pediatric Acute Respiratory Illnesses in Resource-Constrained Settings: a Prospective Cohort Study in Southwestern Uganda
Erratum in
-
Erratum for Ciccone et al., "Rapid Diagnostic Tests to Guide Case Management of and Improve Antibiotic Stewardship for Pediatric Acute Respiratory Illnesses in Resource-Constrained Settings: a Prospective Cohort Study in Southwestern Uganda".Microbiol Spectr. 2022 Feb 23;10(1):e0044322. doi: 10.1128/spectrum.00443-22. Epub 2022 Feb 23. Microbiol Spectr. 2022. PMID: 35196825 Free PMC article. No abstract available.
Abstract
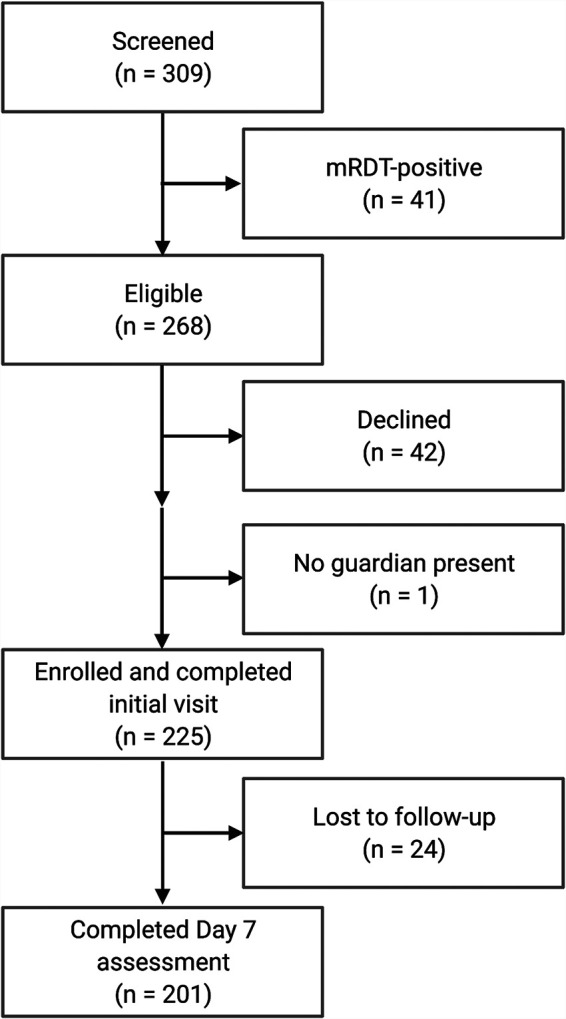
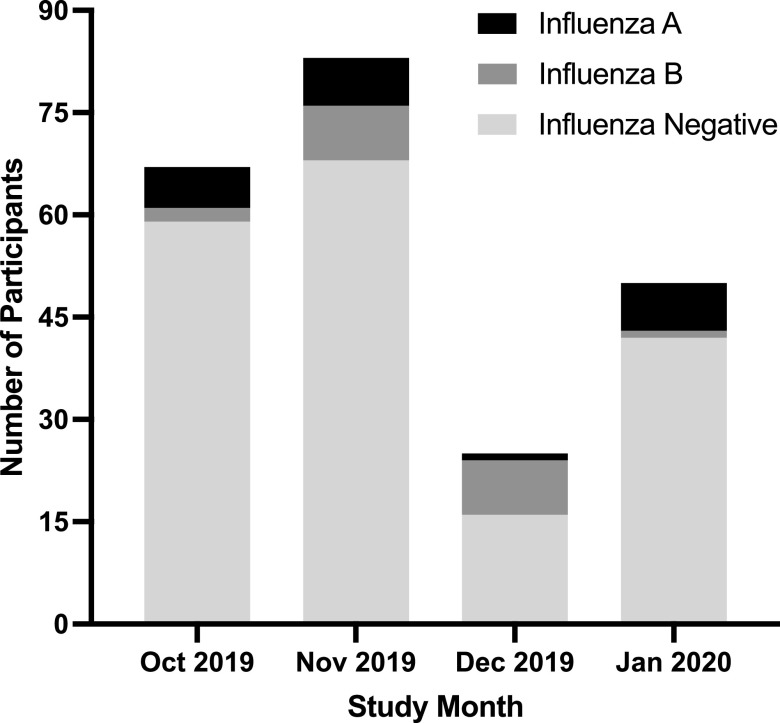
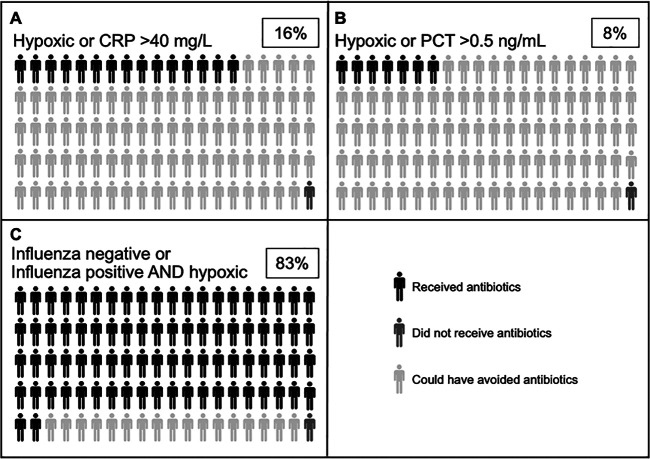
Pediatric acute respiratory illness (ARI) is one of the most common reasons for evaluation at peripheral health centers in sub-Saharan Africa and is frequently managed based on clinical syndrome alone. Although most ARI episodes are likely caused by self-limited viral infections, the majority are treated with antibiotics. This overuse contributes to the development of antimicrobial resistance. To evaluate the preliminary feasibility and potential impact of adding pathogen-specific and clinical biomarker diagnostic testing to existing clinical management algorithms, we conducted a prospective, observational cohort study of 225 children presenting with malaria-negative, febrile ARI to the outpatient department of a semi-urban peripheral health facility in southwestern Uganda from October 2019 to January 2020. In addition to routine clinical evaluation, we performed influenza and Streptococcus pneumoniae antigen testing and measured levels of C-reactive protein, procalcitonin, and lactate in the clinic's laboratory, and conducted a follow-up assessment by phone 7 days later. Almost one-fifth of participants (40/225) tested positive for influenza. Clinical biomarker measurements were low with C-reactive protein of >40 mg/L in only 11% (13/222) of participants and procalcitonin >0.25 ng/mL in only 13% (16/125). All but two children received antibiotic treatment; only 3% (7/225) were admitted. At follow-up, 59% (118/201) of caregivers reported at least one persistent symptom, but fever had resolved for all children. Positive influenza testing was associated with persistent symptoms. In summary, we demonstrate that simple, rapid pathogen-specific testing and biomarker measurement are possible in resource-limited settings and could improve syndromic management and, in turn, antibiotic stewardship. IMPORTANCE Globally, respiratory illness is one of the most common reasons that children seek care. It is often treated inappropriately with antibiotics, which can drive the development of antibiotic resistance. In resource-rich settings, testing for specific pathogens or measurement of clinical biomarkers, such as procalcitonin and C-reactive protein, is often employed to help determine which children should receive antibiotics. However, there are limited data on the use of these tests in resource-constrained, outpatient contexts in sub-Saharan Africa. We enrolled children with respiratory illness presenting to a clinic in southwestern Uganda and performed testing for influenza, Streptococcus pneumoniae, C-reactive protein, and procalcitonin on-site. Almost all children received antibiotics. We demonstrate that employing clinical algorithms that include influenza and clinical biomarker testing could significantly decrease antibiotic prescriptions. Our study therefore provides preliminary data to support the feasibility and potential utility of diagnostics to improve management of respiratory illness in resource-constrained settings.
Keywords: Uganda; antimicrobial stewardship; biomarkers; diagnostics; influenza; pediatric infectious disease; respiratory infections.
Figures
References
-
- World Health Organization. 2021. Maternal, newborn, child and adolescent health and aging data portal. https://www.who.int/data/maternal-newborn-child-adolescent-ageing/child-....
-
- Bruxvoort KJ, Leurent B, Chandler CIR, Ansah EK, Baiden F, Björkman A, Burchett HED, Clarke SE, Cundill B, DiLiberto DD, Elfving K, Goodman C, Hansen KS, Kachur SP, Lal S, Lalloo DG, Leslie T, Magnussen P, Mangham-Jefferies L, Mårtensson A, Mayan I, Mbonye AK, Msellem MI, Onwujekwe OE, Owusu-Agyei S, Rowland MW, Shakely D, Staedke SG, Vestergaard LS, Webster J, Whitty CJM, Wiseman VL, Yeung S, Schellenberg D, Hopkins H. 2017. The impact of introducing malaria rapid diagnostic tests on fever case management: a synthesis of ten studies from the ACT Consortium. Am J Trop Med Hyg 97:1170–1179. doi:10.4269/ajtmh.16-0955. - DOI - PMC - PubMed
-
- Guillebaud J, Bernardson B, Randriambolamanantsoa TH, Randrianasolo L, Randriamampionona JL, Marino CA, Rasolofo V, Randrianarivelojosia M, Vigan-Womas I, Stivaktas V, Venter M, Piola P, Héraud J-M. 2018. Study on causes of fever in primary healthcare center uncovers pathogens of public health concern in Madagascar. PLoS Negl Trop Dis 12:e0006642. doi:10.1371/journal.pntd.0006642. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
