

Biocompatibility and feasibility of VisiPlate, a novel ultrathin, multichannel glaucoma drainage device
- PMID: 34817711
- PMCID: PMC8613174
- DOI: 10.1007/s10856-021-06613-8
Biocompatibility and feasibility of VisiPlate, a novel ultrathin, multichannel glaucoma drainage device
Abstract
Background: Glaucoma is the leading cause of blindness worldwide. Glaucoma drainage devices and minimally invasive glaucoma surgeries (MIGS) often present with tradeoffs in safety and durability of efficacy. Using a rabbit model, we examined the biocompatibility and feasibility of VisiPlate, a novel, ultrathin, tubeless subconjunctival shunt comprised of a network of microchannels.
Methods: Six naive female New Zealand White rabbits received implants (three only in the right eye with contralateral eye untreated and three in both eyes) composed of a 400-nm-thick aluminum oxide core coated with 2 µm of parylene-C, manufactured with microelectromechanical systems (MEMS) techniques. Tonometry, slit lamp exam, clinical exam, fluorescein patency testing, and histopathology were performed.
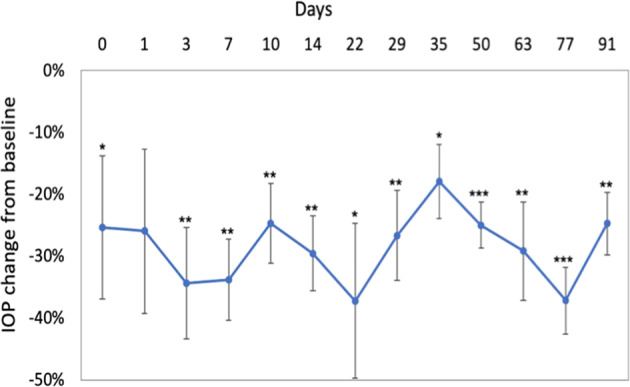
Results: VisiPlate demonstrated IOP-lowering of 20-40% compared to baseline at each time point over the course of 3 months in the nine implanted eyes. All eyes developed blebs over the implant, and fluorescein testing demonstrated fluid patency at 22 days post-implantation. Slit lamp and clinical observations showed that VisiPlate was well tolerated, with low levels of conjunctival congestion, conjunctival swelling, aqueous flare, hyphema, and iris involvement from surgery that resolved over time. At sacrifice time points of 93 days and 180 days, the only notable observations were mild levels of conjunctival congestion in implanted eyes. Histopathology showed minimal tissue response and no obvious inflammation, fibrosis, or necrosis around the implant.
Conclusions: The results of this in vivo study demonstrate the biocompatibility and IOP-lowering effect of a multichannel, ultrathin subconjunctival shunt in a rabbit model. The data suggest that VisiPlate may safely enhance aqueous outflow and significantly reduce intraocular pressure.
© 2021. The Author(s).
Conflict of interest statement
BWK: commercial relationship with Avisi Technologies, Co-Founder Avisi Technologies. EM: N/A. Thomas Barbolt: Commercial Relationship with Avisi Technologies, Consultant, Advisory Board. RAL: commercial relationship with Avisi Technologies, Advisory Board . IIA: commercial relationship with Avisi Technologies, Advisory Board. VL: commercial relationship with Avisi Technologies, Advisory Board. SMN: commercial relationship with Avisi Technologies, Consultant, Advisory Board. GG: commercial relationship with Avisi Technologies, VP Research and Development. EGM-E: Commercial Relationship with Avisi Technologies, Consultant, Advisory Board
Figures




References
-
- Tham Y-C, Li X, Wong TY, Quigley HA, Aung T, Cheng C-Y. Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis. Ophthalmology. 2014;121:2081–90. 10.1016/j.ophtha.2014.05.013. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
