

Communicating imaging findings in peritoneal mesothelioma: the impact of 'PAUSE' on surgical decision-making
- PMID: 34817720
- PMCID: PMC8613330
- DOI: 10.1186/s13244-021-01118-y
Communicating imaging findings in peritoneal mesothelioma: the impact of 'PAUSE' on surgical decision-making
Abstract
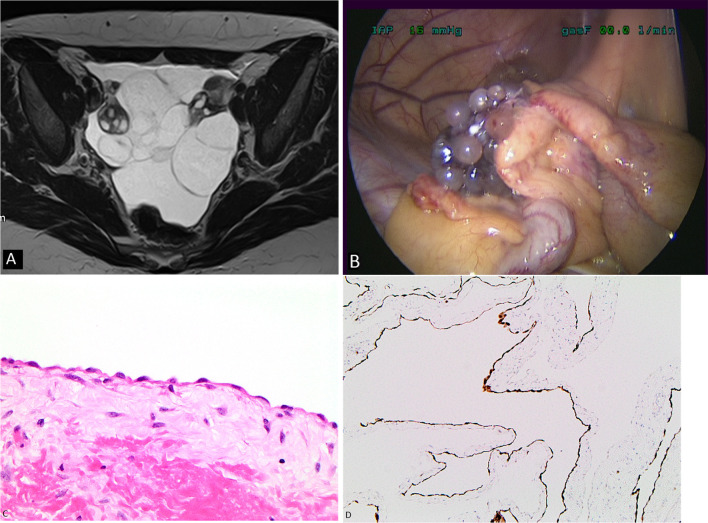
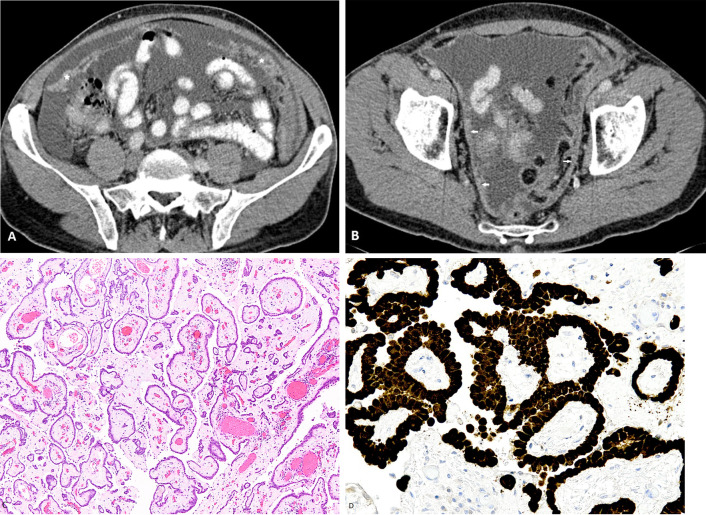
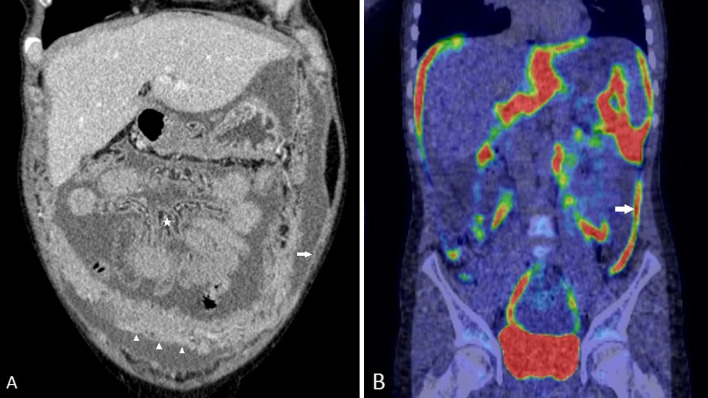
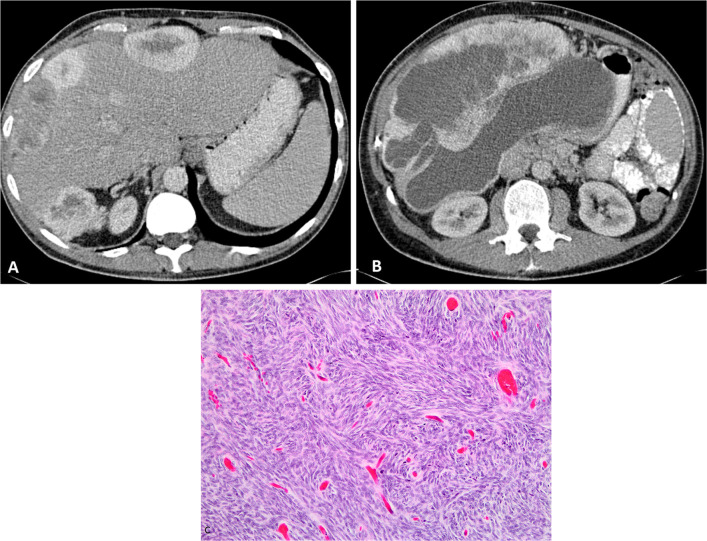
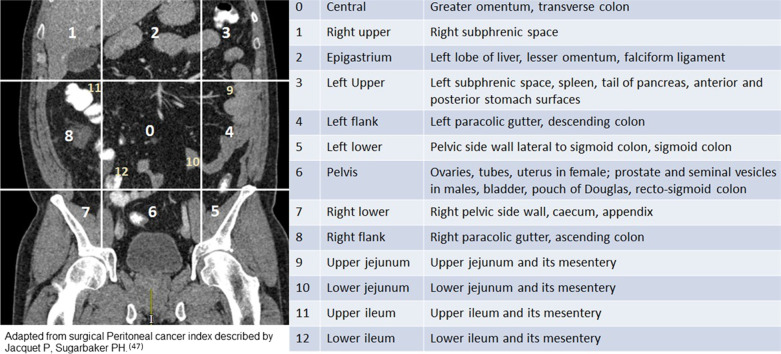
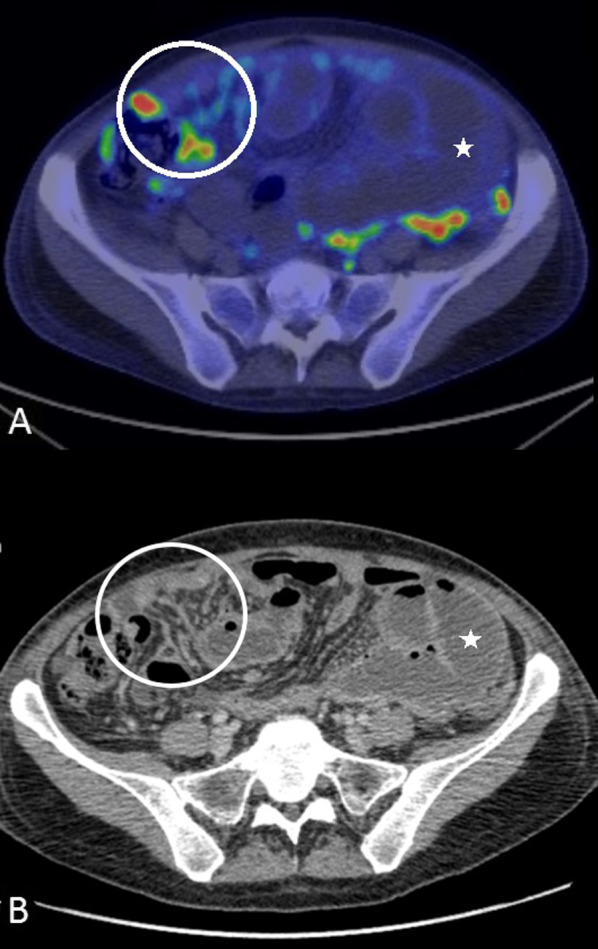
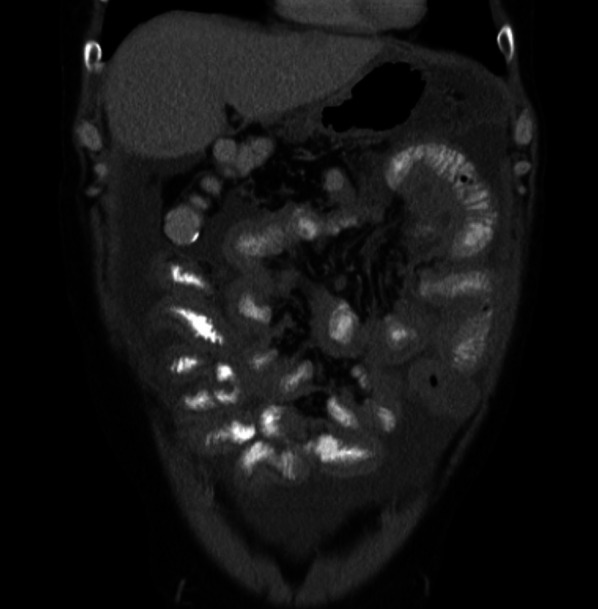
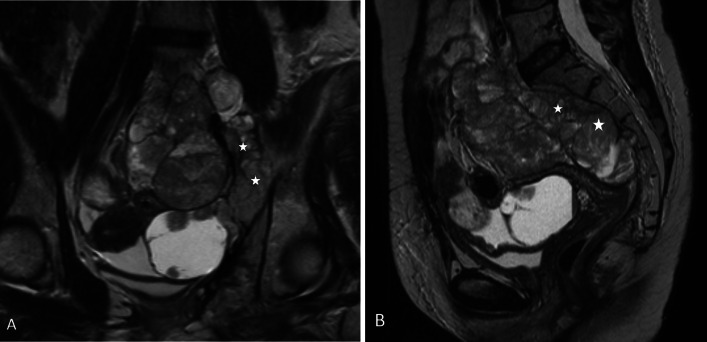
The peritoneal cavity is the second commonest site of mesothelioma after the pleural cavity. There are five histological types of peritoneal mesothelioma with variable symptomatology, clinical presentation and prognosis. Cystic mesothelioma is a borderline malignant neoplasm with a favourable prognosis, well-differentiated papillary mesothelioma is generally a low-grade malignancy, and all other varieties such as epithelioid, sarcomatoid and biphasic mesothelioma are highly malignant types of peritoneal mesothelioma with poor prognosis. Malignant peritoneal mesothelioma was considered inevitably fatal prior to the introduction of cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC) in selected cases where long-term survival and cure could be achieved. However, the survival benefits following CRS and HIPEC mainly depend on completeness of cytoreduction, which come at the cost of high morbidity and potential mortality. Using the acronym 'PAUSE', we aimed at describing the key imaging findings that impact surgical decision-making in patients with peritoneal mesothelioma. PAUSE stands for peritoneal cancer index, ascites and abdominal wall disease, unfavourable sites of involvement, small bowel and mesenteric disease and extraperitoneal disease. Reporting components of 'PAUSE' is crucial for patient selection. Despite limitations of CT in accurately depicting the volume of disease, describing findings in terms of PAUSE plays an important role in excluding patients who might not benefit from CRS and HIPEC.
Keywords: Complete cytoreduction; Imaging; PAUSE; Peritoneal mesothelioma; Radiological peritoneal cancer index.
© 2021. The Author(s).
Conflict of interest statement
The authors have no financial or proprietary interests in any material discussed in this article.
Figures










References
Publication types
LinkOut - more resources
Full Text Sources
