

Budget impact of lasmiditan for the acute treatment of migraine in the United States
- PMID: 34818093
- PMCID: PMC10391167
- DOI: 10.18553/jmcp.2021.27.12.1714
Budget impact of lasmiditan for the acute treatment of migraine in the United States
Abstract
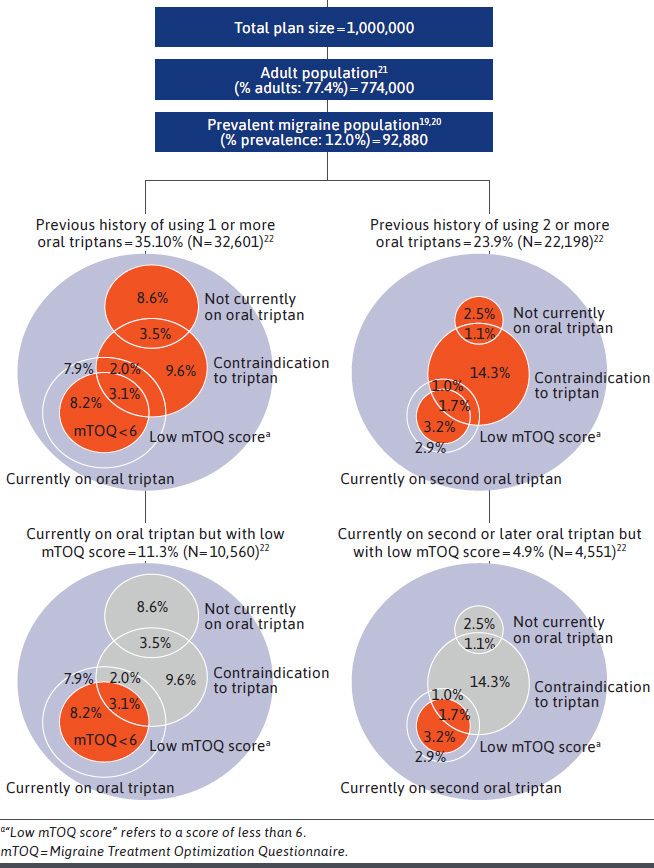
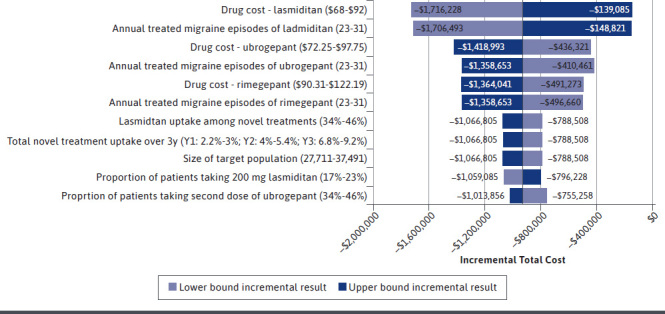
BACKGROUND: Three novel acute treatments for migraine-lasmiditan, ubrogepant, and rimegepant-were approved by the FDA in 2019 and 2020 for adults with migraine with and without aura. American Headache Society guidance recommends that these novel acute treatments be considered for patients who are contraindicated to or fail to respond or tolerate oral triptans, the current standard of acute care. OBJECTIVE: To estimate, from a US commercial plan perspective, the budget impact of adding lasmiditan as an option to a formulary that already includes ubrogepant and rimegepant. METHODS: Epidemiologic data were drawn from US Census data, the American Migraine Prevalence and Preventive study, and the first wave of the OVERCOME US survey, a web-based survey that included 21,000 patients with migraine. A model with a 3-year time horizon was built assuming that demand for the novel acute treatments would not vary based on whether lasmiditan is included in the formulary. The model examined a variety of populations, in particular beneficiaries with previous use of 1 or more oral triptans or contraindicated to triptans and beneficiaries with previous use of 2 or more oral triptans or contraindicated to triptans. Primary outcomes were the incremental differences in total cost and average cost per member per month (PMPM) between scenarios with and without lasmiditan. One-way sensitivity analyses with model parameters that were varied by plus or minus 15% were conducted to assess the effect of key parameters on the incremental total cost over 3 years. RESULTS: The addition of lasmiditan to a formulary that already includes ubrogepant and rimegepant resulted in a total savings of -$927,657 (-1.5% compared with the scenario without lasmiditan) over a 3-year time horizon in the population with previous history of using 1 or more oral triptans or contraindicated to a triptan. In the population with previous history of using 2 or more oral triptans or contraindicated, the addition of lasmiditan resulted in a total budget impact of -$466,518 (-1.3%) over a 3-year time horizon. Most of the cost savings was attributable to reductions in drug acquisition cost. Savings in total costs resulted in average incremental cost per PMPM of -0.03 and -$0.01, respectively. CONCLUSIONS: The addition of lasmiditan to the formulary as a novel acute treatment option for migraine alongside ubrogepant and rimegepant resulted in lower budget impact on a 3-year time horizon from a US commercial payer's perspective. This result is important to US commercial payers as they seek to incorporate the emerging novel acute treatments for migraine into their benefit designs. DISCLOSURES: This work was funded by Eli Lilly and Company. Milev and Sun are employed by Evidera, which received funding from Eli Lilly and Company for work on this project. Pohl, Mason, Njuguna, and Loo are employees and stockholders of Eli Lilly and Company.
Conflict of interest statement
This work was funded by Eli Lilly and Company. Milev and Sun are employed by Evidera, which received funding from Eli Lilly and Company for work on this project. Pohl, Mason, Njuguna, and Loo are employees and stockholders of Eli Lilly and Company.
Figures
References
-
- Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd edition. Cephalalgia. 2018;38(1):1-211. - PubMed
-
- Woldeamanuel YW, Cowan RP. Migraine affects 1 in 10 people worldwide featuring recent rise: A systematic review and meta-analysis of community-based studies involving 6 million participants. J Neurol Sci. 2017;372:307-315. - PubMed
-
- Lipton RB, Stewart WF, Diamond S, Diamond ML, Reed M. Prevalence and burden of migraine in the United States: data from the American Migraine Study II. Headache. 2001;41(7):646-57. - PubMed
-
- Burch RC, Loder S, Loder E, Smitherman TA. The prevalence and burden of migraine and severe headache in the United States: updated statistics from government health surveillance studies. Headache. 2015;55(1):21-34. - PubMed
-
- Burshtein R, Burshtein A, Burshtein J, Rosen N. Are episodic and chronic migraine one disease or two? Curr Pain Headache Rep. 2015;19(12):53. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
