

PERG adaptation for detection of retinal ganglion cell dysfunction in glaucoma: a pilot diagnostic accuracy study
- PMID: 34819533
- PMCID: PMC8613213
- DOI: 10.1038/s41598-021-02048-x
PERG adaptation for detection of retinal ganglion cell dysfunction in glaucoma: a pilot diagnostic accuracy study
Abstract
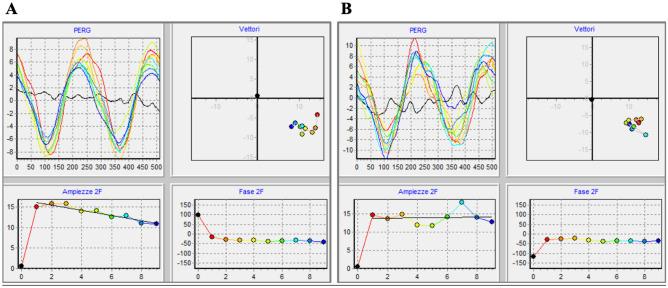
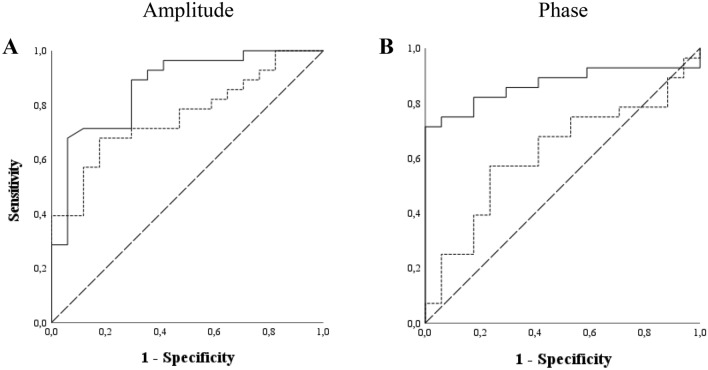
It has been previously demonstrated that the adaptive phase changes of steady-state pattern electroretinogram (SS-PERG), recorded during 4-min presentation of patterned stimuli, are reduced in glaucoma suspects and patients compared to normal subjects. Our study aims at testing the hypothesis that adaptive changes of SS-PERG, recorded using the novel optimized Next Generation PERG (PERGx) protocol, differ between glaucoma patients and controls. In this pilot cross-sectional study, we included 28 glaucoma patients and 17 age-matched normal subjects. Both patients and controls underwent a full ophthalmologic examination, visual field testing, OCT and PERGx. The PERGx signal was sampled over 2 min (providing 1 noise and 9 signal packets) in response to alternating gratings generated on an OLED display. PERGx amplitude and phase were analyzed to quantify adaptive changes over recording time. Receiver operating characteristic (ROC) curves were used to study the diagnostic accuracy of PERGx parameters in distinguishing glaucoma patients from normal subjects. PERGx amplitude and phase data showed declining trends in both groups. PERGx amplitude slope and grand-average vector amplitude and phase were significantly different in patients compared to controls (p < 0.01), whereas phase angular dispersion was greater in patients but not significantly different between the two groups. The area under the ROC curves were 0.87 and 0.76 for PERGx amplitude slope and grand-average vector amplitude, and 0.62 and 0.87 for PERGx angular dispersion and grand-average vector phase, respectively. The PERGx paradigm resulted highly accurate in detecting the reduction of amplitude adaptive changes in glaucoma patients, presumably due to the loss of functional retinal ganglion cell autoregulation. Thus, PERG adaptation, recorded by this new protocol, might be helpful in the identification and diagnosis of early glaucomatous dysfunction.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
