

Mandibular Fractures: Diagnosis and Management
- PMID: 34819805
- PMCID: PMC8604616
- DOI: 10.1055/s-0041-1735818
Mandibular Fractures: Diagnosis and Management
Abstract
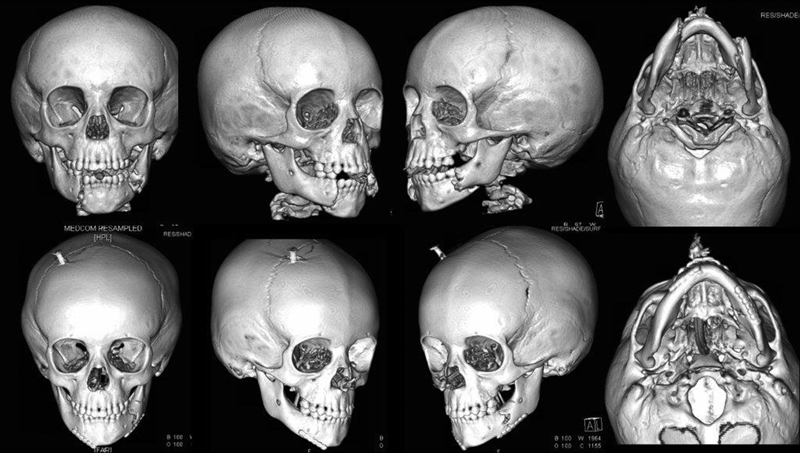
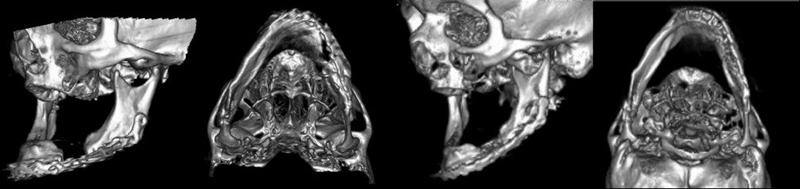
Accurate evaluation, diagnosis, and management of mandibular fractures is essential to effectively restore an individual's facial esthetics and function. Understanding of surgical anatomy, fracture fixation principles, and the nuances of specific fractures with respect to various patient populations can aid in adequately avoiding complications such as malocclusion, non-union, paresthesia, and revision procedures. This article reviews comprehensive mandibular fracture assessment, mandibular surgical anatomy, fracture fixation principles, management considerations, and commonly encountered complications. In addition, this article reviews emerging literature examining 3-dimensional printing and intraoperative imaging.
Keywords: craniomaxillofacial trauma; facial trauma; mandible; mandibular fracture; maxillofacial injury.
Thieme. All rights reserved.
Conflict of interest statement
Conflict of Interest None declared.
Figures





References
-
- Kim K, Ibrahim A MS, Koolen P GL, Lee B T, Lin S J. Trends in facial fracture treatment using the American College of Surgeons National Surgical Quality Improvement Program database. Plast Reconstr Surg. 2014;133(03):627–638. - PubMed
-
- Afrooz P N, Bykowski M R, James I B, Daniali L N, Clavijo-Alvarez J A. The Epidemiology of Mandibular Fractures in the United States, Part 1: A Review of 13,142 Cases from the US National Trauma Data Bank. J Oral Maxillofac Surg. 2015;73(12):2361–2366. - PubMed
-
- Iida S, Kogo M, Sugiura T, Mima T, Matsuya T. Retrospective analysis of 1502 patients with facial fractures. Int J Oral Maxillofac Surg. 2001;30(04):286–290. - PubMed
