

Liposomal irinotecan pre-emptive dose reduction in patients with pancreatic ductal adenocarcinoma: 667 patients' experience within a population-based study
- PMID: 34819998
- PMCID: PMC8606735
- DOI: 10.1177/17588359211058255
Liposomal irinotecan pre-emptive dose reduction in patients with pancreatic ductal adenocarcinoma: 667 patients' experience within a population-based study
Abstract
Background: Liposomal irinotecan (nal-IRI) plus 5-fluorouracil and leucovorin (5-FU/LV) is currently the standard second-line treatment for patients with pancreatic ductal adenocarcinoma (PDAC) after previous failed gemcitabine-based therapy. This population-based study aimed to evaluate the efficacy and safety of nal-IRI + 5-FU/LV and the association of pre-emptive nal-IRI dosing with treatment outcomes in patients with PDAC.
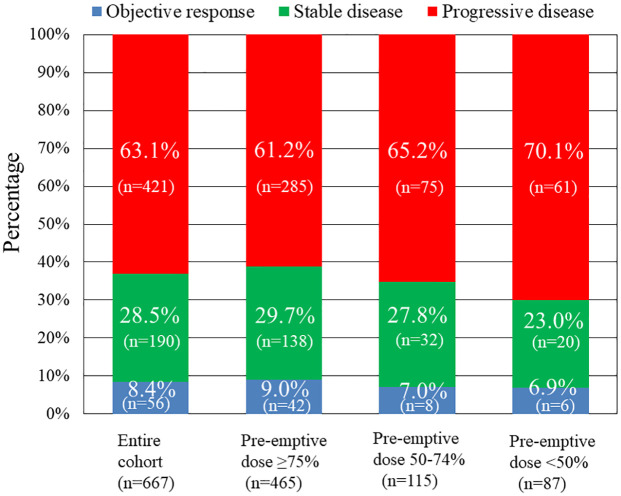
Methods: We retrospectively enrolled a total of 667 consecutive patients with PDAC who received nal-IRI plus 5-FU/LV treatment between August 2018 and November 2020 at 9 medical centers in Taiwan. Patients were allocated into groups according to pre-emptive nal-IRI dosing (⩾75%, 50-74%, <50%) for comparison of treatment efficacy and safety.
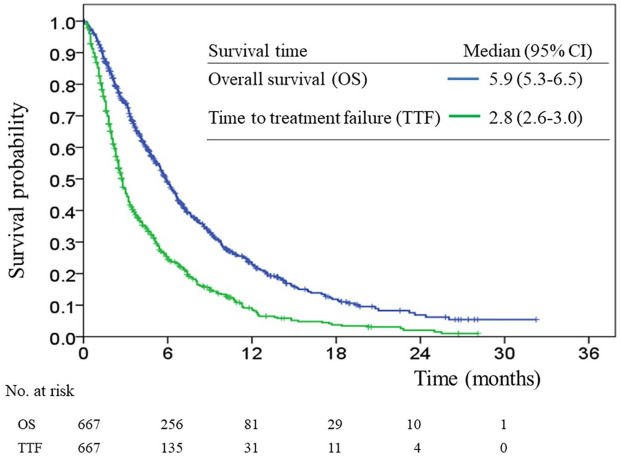
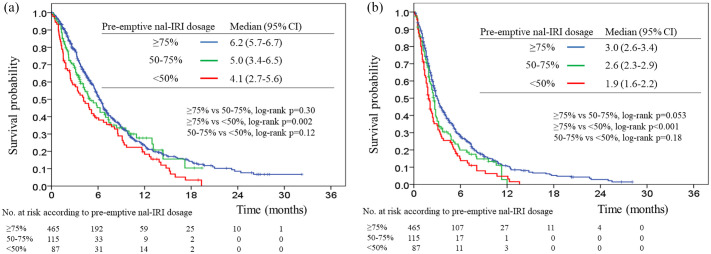
Results: The median overall survival (OS) and time to treatment failure (TTF) were 5.9 months [95% confidence interval (CI), 5.3-6.5] and 2.8 months (95% CI, 2.6-3.0), respectively. The median OS was 6.5 months (95% CI, 5.7-6.7), 5.0 months (95% CI, 3.4-6.5), and 4.1 months (95% CI, 2.7-5.6), respectively, among the ⩾75%, 50-74%, and <50% pre-emptive nal-IRI dosing groups, whereas the median TTF of the three groups was 3.0 months (95% CI, 2.6-3.4), 2.6 months (95% CI, 2.3-2.9), and 1.9 months (95% CI, 1.6-2.2), respectively. Pre-emptive nal-IRI dosing <50% was an independent negative prognostic factor for OS and TTF in multivariate analyses. The most common severe adverse events were neutropenia (22.9%), anemia (21.1%), and hypokalemia (15.4%). Patients in the <50% pre-emptive nal-IRI dosing group had a significantly lower incidence of neutropenia and non-neutropenic infection than those in the other groups.
Conclusion: Our results support the use of nal-IRI + 5-FU/LV as standard clinical practice for treating patients with PDAC based on this large population-based study. Our findings encourage physicians to provide adequate doses of nal-IRI in order to achieve better outcomes without compromising safety profiles.
Keywords: dose reduction; liposomal irinotecan; outcome; pancreatic cancer; toxicity.
© The Author(s), 2021.
Conflict of interest statement
Conflict of interest statement: The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
Similar articles
-
The impact of starting dose with or without subsequent dose escalation of liposomal irinotecan on treatment outcomes in patients with metastatic pancreatic ductal adenocarcinoma.Am J Cancer Res. 2022 Nov 15;12(11):5062-5073. eCollection 2022. Am J Cancer Res. 2022. PMID: 36504882 Free PMC article.
-
Nanoliposomal irinotecan plus fluorouracil and folinic acid as a second-line treatment option in patients with metastatic pancreatic ductal adenocarcinoma: a retrospective cohort study.BMC Cancer. 2021 Nov 3;21(1):1176. doi: 10.1186/s12885-021-08887-1. BMC Cancer. 2021. PMID: 34732161 Free PMC article.
-
Validation of a Prognostic Nomogram for Patients with Metastatic Pancreatic Cancer Treated with Nanoliposomal Irinotecan as Second-Line Therapy.Cancer Control. 2025 Jan-Dec;32:10732748251333040. doi: 10.1177/10732748251333040. Epub 2025 Apr 11. Cancer Control. 2025. PMID: 40216411 Free PMC article.
-
Development of nanoliposomal irinotecan (nal-IRI, MM-398, PEP02) in the management of metastatic pancreatic cancer.Expert Opin Pharmacother. 2016 Jul;17(10):1413-20. doi: 10.1080/14656566.2016.1183646. Epub 2016 May 17. Expert Opin Pharmacother. 2016. PMID: 27140876 Review.
-
Liposomal Irinotecan: A Review in Metastatic Pancreatic Adenocarcinoma.Drugs. 2020 Jul;80(10):1007-1018. doi: 10.1007/s40265-020-01336-6. Drugs. 2020. PMID: 32557396 Free PMC article. Review.
Cited by
-
Systemic treatments in pancreatic cancer: Taiwan pancreas society recommendation.Biomed J. 2024 Jun;47(3):100696. doi: 10.1016/j.bj.2023.100696. Epub 2023 Dec 31. Biomed J. 2024. PMID: 38169173 Free PMC article. Review.
-
Relationship between neutropenia caused by nanoliposomal irinotecan/fluorouracil/leucovorin and treatment outcomes in the NAPOLEON-2 study (NN-2301).Sci Rep. 2025 Jan 27;15(1):3427. doi: 10.1038/s41598-025-88005-4. Sci Rep. 2025. PMID: 39870769 Free PMC article.
-
The impact of starting dose with or without subsequent dose escalation of liposomal irinotecan on treatment outcomes in patients with metastatic pancreatic ductal adenocarcinoma.Am J Cancer Res. 2022 Nov 15;12(11):5062-5073. eCollection 2022. Am J Cancer Res. 2022. PMID: 36504882 Free PMC article.
-
Outcomes of Liposomal Irinotecan With 5-FU and Leucovorin in Patients With Metastatic Pancreatic Cancer and Borderline Performance Status.Cancer Diagn Progn. 2025 Mar 3;5(2):198-206. doi: 10.21873/cdp.10430. eCollection 2025 Mar-Apr. Cancer Diagn Progn. 2025. PMID: 40034960 Free PMC article.
-
Predictive value of albumin combined with neutrophil-to-lymphocyte ratio for efficacy and safety profiles in patients with pancreatic ductal adenocarcinoma receiving liposomal irinotecan plus 5-fluorouracil and leucovorin.Am J Cancer Res. 2022 Sep 15;12(9):4267-4278. eCollection 2022. Am J Cancer Res. 2022. PMID: 36225629 Free PMC article.
References
-
- Sung H, Ferlay J, Siegel RL, et al.. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021; 71: 209–249. - PubMed
-
- Ryan DP, Hong TS, Bardeesy N. Pancreatic adenocarcinoma. N Engl J Med 2014; 371: 1039–1049. - PubMed
-
- Moore MJ, Goldstein D, Hamm J, et al.. Erlotinib plus gemcitabine compared with gemcitabine alone in patients with advanced pancreatic cancer: a phase III trial of the National Cancer Institute of Canada Clinical Trials Group. J Clin Oncol 2007; 25: 1960–1966. - PubMed
-
- Conroy T, Desseigne F, Ychou M, et al.. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med 2011; 364: 1817–1825. - PubMed
LinkOut - more resources
Full Text Sources
