

Hybrid Transtibial Femoral Preparation for Transphyseal Anterior Cruciate Ligament Reconstruction: A Radiographic Comparison With the Transtibial and Anteromedial Portal Techniques
- PMID: 34820462
- PMCID: PMC8607486
- DOI: 10.1177/23259671211054509
Hybrid Transtibial Femoral Preparation for Transphyseal Anterior Cruciate Ligament Reconstruction: A Radiographic Comparison With the Transtibial and Anteromedial Portal Techniques
Abstract
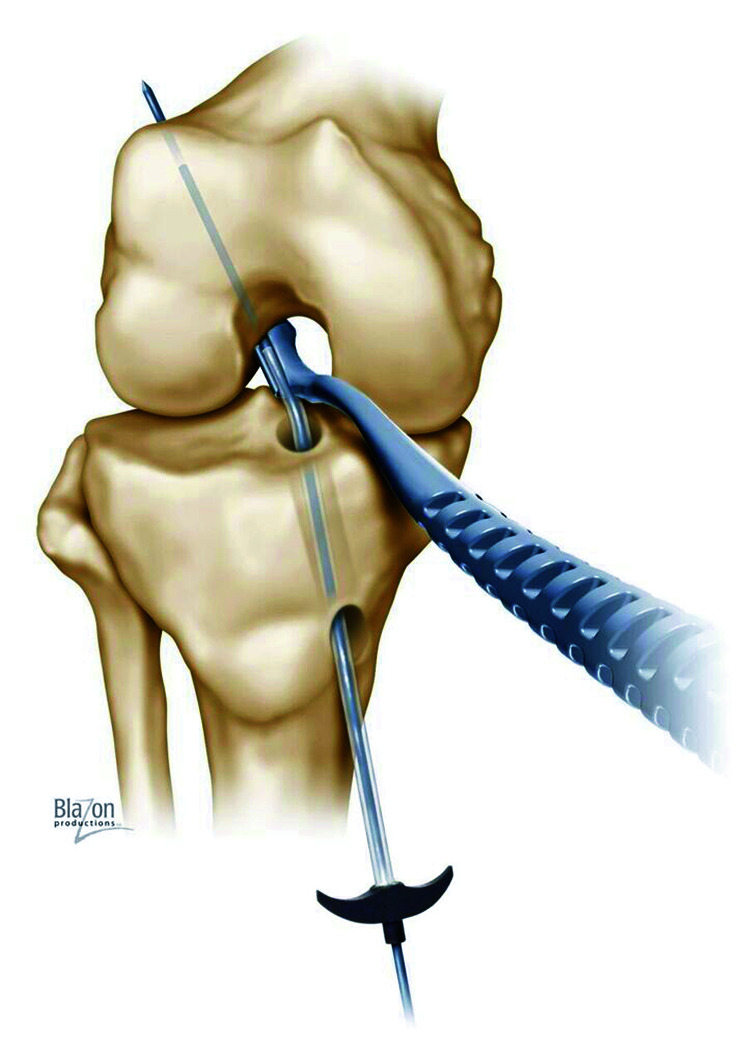
Background: Transphyseal anterior cruciate ligament (ACL) reconstruction remains the most commonly used technique for pubescent patients. The transtibial (TT) drilling technique creates vertical and central femoral tunnels to minimize the physeal area of injury at the expense of a nonanatomic femoral tunnel. The hybrid TT (HTT) technique offers the potential of an anatomic femoral position with tunnel geometry similar to that using the TT technique.
Purpose/hypothesis: The purpose was to perform a radiographic comparison of the HTT technique with TT and anteromedial portal (AM) techniques in adolescent patients undergoing transphyseal ACL reconstruction. It was hypothesized that femoral tunnels created during HTT would be similar to TT tunnels but significantly more vertical and central than AM tunnels.
Study design: Cohort study; Level of evidence, 3.
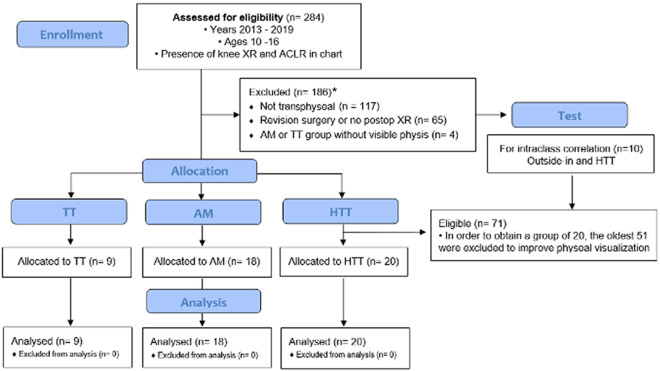
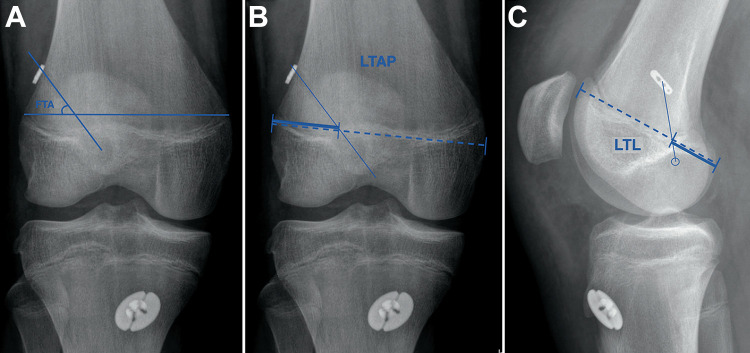
Methods: We retrospectively screened primary transphyseal ACL reconstructions performed in adolescents at our institution between 2013 and 2019. The youngest 20 eligible patients were selected from each technique cohort: TT, AM, and HTT. Postoperative radiographs were assessed for the coronal femoral tunnel angle, as well as the location of the tunnel-physis penetration on the anteroposterior and lateral views. Physeal lesion surface area was calculated. Data were compared among the 3 groups using 1-way analysis of variance followed by pairwise comparisons.
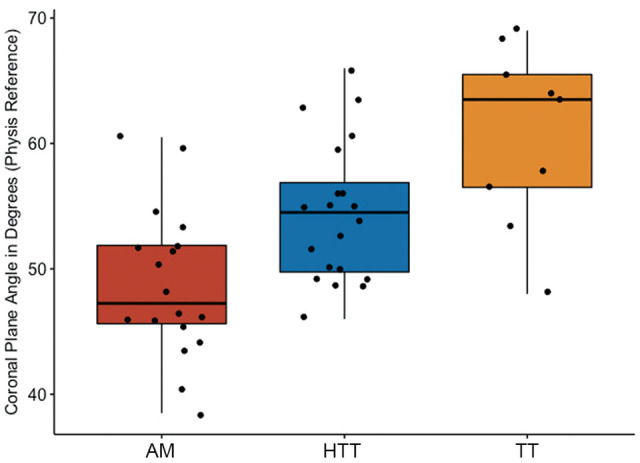
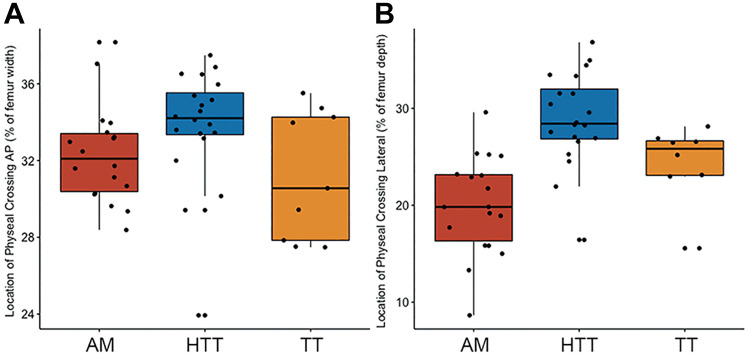
Results: Included were 47 patients with a mean ± SD age of 14.3 ± 1.2 years (n = 9 with TT, 18 with AM, and 20 with HTT techniques). The coronal tunnel angle was significantly more vertical in the TT (60.7° ± 7.2°) and HTT (54.4° ± 5.7) groups as compared with the AM group (48.8° ± 5.9; P = .0037 and P = .02, respectively). There was no significant difference between the TT and HTT groups (P = .066). The only significant finding regarding femoral tunnel location was that the HTT tunnels (28.9% ± 4.8%) penetrated the physis more centrally than did the AM tunnels (20.0% ± 5.1%; P = .00002) on lateral radiographs.
Conclusion: The HTT technique presents an option for transphyseal ACL reconstruction, with femoral tunnel obliquity and estimated physeal disruption similar to that of the TT technique and significantly less than that of the AM technique. The HTT technique also results in the most central physeal perforation of all techniques, predominantly in the sagittal plane.
Keywords: ACL; anatomy; pediatric sports medicine; physis.
© The Author(s) 2021.
Conflict of interest statement
One or more of the authors has declared the following potential conflict of interest or source of funding: J.C.R. has received research support from Biopharma, consulting fees from Stryker, and hospitality payments from Smith & Nephew and has stock/stock options in Resor3d. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Figures
Similar articles
-
A Hybrid Transtibial Technique Combines the Advantages of Anteromedial Portal and Transtibial Approaches: A Prospective Randomized Controlled Trial.Am J Sports Med. 2020 Nov;48(13):3200-3207. doi: 10.1177/0363546520956645. Epub 2020 Oct 5. Am J Sports Med. 2020. PMID: 33017169 Clinical Trial.
-
Transphyseal ACL Reconstruction in Skeletally Immature Patients: Does Independent Femoral Tunnel Drilling Place the Physis at Greater Risk Compared With Transtibial Drilling?Orthop J Sports Med. 2016 Jun 7;4(6):2325967116650432. doi: 10.1177/2325967116650432. eCollection 2016 Jun. Orthop J Sports Med. 2016. PMID: 27331075 Free PMC article.
-
Comparison of Growth Plate Violations for Transtibial and Anteromedial Surgical Techniques in Simulated Adolescent Anterior Cruciate Ligament Reconstruction.Am J Sports Med. 2016 Feb;44(2):417-24. doi: 10.1177/0363546515619624. Epub 2015 Dec 18. Am J Sports Med. 2016. PMID: 26684661
-
Clinical and Radiological Outcomes of Anteromedial Portal Versus Transtibial Technique in ACL Reconstruction: A Systematic Review.Orthop J Sports Med. 2021 Jul 2;9(7):23259671211024591. doi: 10.1177/23259671211024591. eCollection 2021 Jul. Orthop J Sports Med. 2021. PMID: 34277881 Free PMC article. Review.
-
Femoral tunnel widening is similar between anteromedial portal and transtibial techniques following single-bundle anterior cruciate ligament reconstruction: a systematic review and meta-analysis.Knee Surg Sports Traumatol Arthrosc. 2019 Feb;27(2):626-635. doi: 10.1007/s00167-018-5204-z. Epub 2018 Oct 10. Knee Surg Sports Traumatol Arthrosc. 2019. PMID: 30306239
Cited by
-
The Hybrid Transtibial Technique Using the LARS Device in Primary Anterior Cruciate Ligament Reconstruction.Video J Sports Med. 2023 Jul 19;3(4):26350254231176827. doi: 10.1177/26350254231176827. eCollection 2023 Jul-Aug. Video J Sports Med. 2023. PMID: 40308678 Free PMC article.
-
Anatomic femoral tunnel and satisfactory clinical outcomes achieved with the modified transtibial technique in anterior cruciate ligament reconstruction: A systematic review and meta-analysis.Heliyon. 2024 Aug 6;10(16):e35824. doi: 10.1016/j.heliyon.2024.e35824. eCollection 2024 Aug 30. Heliyon. 2024. PMID: 39224330 Free PMC article.
References
-
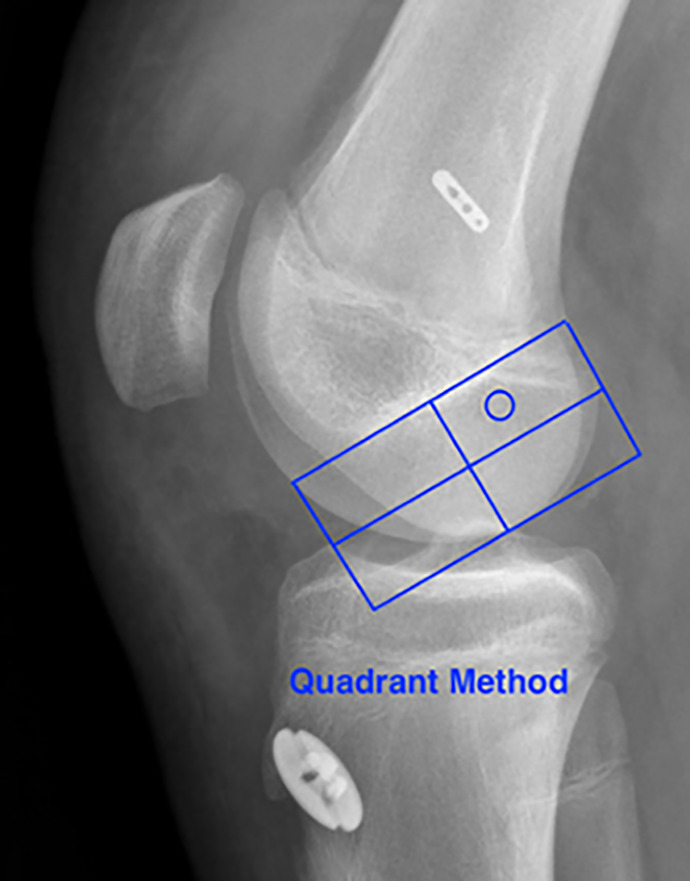
- Bernard M, Hertel P, Hornung H, Cierpinski T. Femoral insertion of the ACL Radiographic quadrant method. Am J Knee Surg. 1997 Winter;10(1):14–21; discussion 21-2. - PubMed
-
- Bhatia S, Korth K, Van Thiel GS, et al. Effect of tibial tunnel diameter on femoral tunnel placement in transtibial single bundle ACL reconstruction. Knee Surg Sports Traumatol Arthrosc. 2016;24(1):51–57. - PubMed
-
- Dodwell ER, Lamont LE, Green DW, Pan TJ, Marx RG, Lyman S. 20 Years of pediatric anterior cruciate ligament reconstruction in New York State. Am J Sports Med. 2014;42(3):675–680. - PubMed
-
- Gausden EB, Calcei JG, Fabricant PD, Green DW. Surgical options for anterior cruciate ligament reconstruction in the young child. Curr Opin Pediatr. 2015;27(1):82–91. - PubMed
LinkOut - more resources
Full Text Sources
