

Metabolite profiles and the risk of metabolic syndrome in early childhood: a case-control study
- PMID: 34823524
- PMCID: PMC8616718
- DOI: 10.1186/s12916-021-02162-7
Metabolite profiles and the risk of metabolic syndrome in early childhood: a case-control study
Abstract
Background: Defining the metabolic syndrome (MetS) in children remains challenging. Furthermore, a dichotomous MetS diagnosis can limit the power to study associations. We sought to characterize the serum metabolite signature of the MetS in early childhood using high-throughput metabolomic technologies that allow comprehensive profiling of metabolic status from a biospecimen.
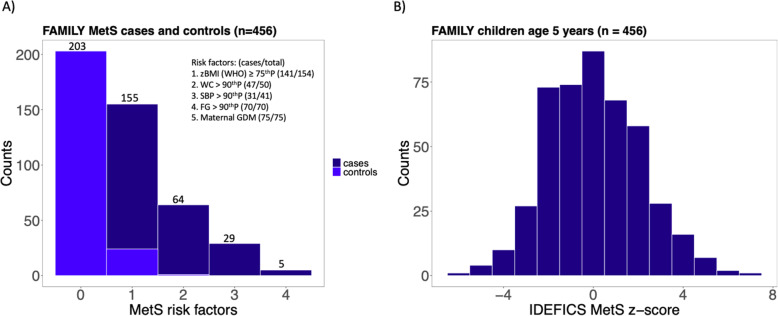
Methods: In the Family Atherosclerosis Monitoring In earLY life (FAMILY) prospective birth cohort study, we selected 228 cases of MetS and 228 matched controls among children age 5 years. In addition, a continuous MetS risk score was calculated for all 456 participants. Comprehensive metabolite profiling was performed on fasting serum samples using multisegment injection-capillary electrophoresis-mass spectrometry. Multivariable regression models were applied to test metabolite associations with MetS adjusting for covariates of screen time, diet quality, physical activity, night sleep, socioeconomic status, age, and sex.
Results: Compared to controls, thirteen serum metabolites were identified in MetS cases when using multivariable regression models, and using the quantitative MetS score, an additional eight metabolites were identified. These included metabolites associated with gluconeogenesis (glucose (odds ratio (OR) 1.55 [95% CI 1.25-1.93]) and glutamine/glutamate ratio (OR 0.82 [95% CI 0.67-1.00])) and the alanine-glucose cycle (alanine (OR 1.41 [95% CI 1.16-1.73])), amino acids metabolism (tyrosine (OR 1.33 [95% CI 1.10-1.63]), threonine (OR 1.24 [95% CI 1.02-1.51]), monomethylarginine (OR 1.33 [95% CI 1.09-1.64]) and lysine (OR 1.23 [95% CI 1.01-1.50])), tryptophan metabolism (tryptophan (OR 0.78 [95% CI 0.64-0.95])), and fatty acids metabolism (carnitine (OR 1.24 [95% CI 1.02-1.51])). The quantitative MetS risk score was more powerful than the dichotomous outcome in consistently detecting this metabolite signature.
Conclusions: A distinct metabolite signature of pediatric MetS is detectable in children as young as 5 years old and may improve risk assessment at early stages of development.
Keywords: Amino acids metabolism; Cardiometabolic risk factors; Continuous risk score; Early childhood; Fatty acids metabolism; Gluconeogenesis; Metabolic syndrome; Metabolomics; Tyrosine and alanine.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Anand SS, Yi Q, Gerstein H, Lonn E, Jacobs R, Vuksan V, Teo K, Davis B, Montague P, Yusuf S, Study of Health Assessment and Risk in Ethnic Groups. Study of Health Assessment and Risk Evaluation in Aboriginal Peoples Investigators Relationship of metabolic syndrome and fibrinolytic dysfunction to cardiovascular disease. Circulation. 2003;108(4):420–425. doi: 10.1161/01.CIR.0000080884.27358.49. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
