

Selexipag for the treatment of chronic thromboembolic pulmonary hypertension
- PMID: 34824052
- PMCID: PMC9260121
- DOI: 10.1183/13993003.01694-2021
Selexipag for the treatment of chronic thromboembolic pulmonary hypertension
Abstract
Background: Treatment options for inoperable chronic thromboembolic pulmonary hypertension (CTEPH) remain limited. Selexipag, an oral selective IP prostacyclin receptor agonist approved for pulmonary arterial hypertension, is a potential treatment option for CTEPH.
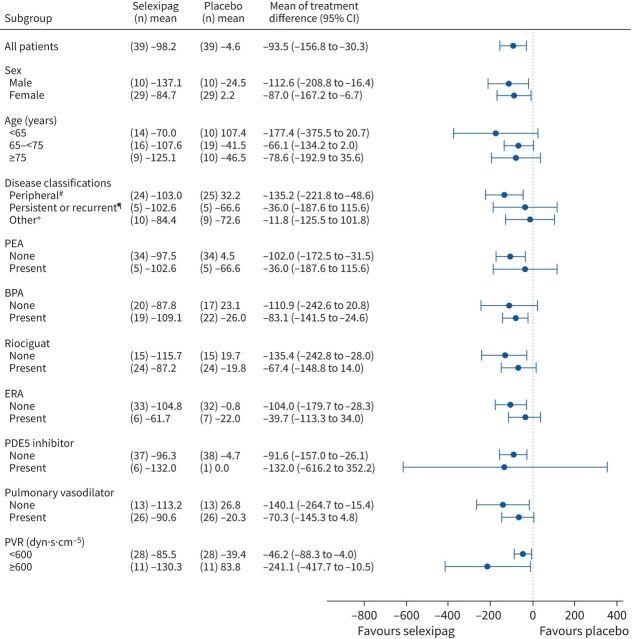
Methods: In this multicentre, randomised, double-blind, placebo-controlled study, 78 Japanese patients with inoperable CTEPH or persistent/recurrent pulmonary hypertension after pulmonary endarterectomy and/or balloon pulmonary angioplasty were randomly assigned to receive placebo or selexipag. The primary end-point was the change in pulmonary vascular resistance (PVR) from baseline to week 20. Secondary end-points were changes in other haemodynamic parameters: 6-min walk distance (6MWD), Borg dyspnoea scale score, World Health Organization (WHO) functional class, EuroQol five-dimension five-level tool and N-terminal pro-brain natriuretic peptide.
Results: The change in PVR was -98.2±111.3 dyn·s·cm-5 and -4.6±163.6 dyn·s·cm-5 in the selexipag and placebo groups, respectively (mean difference -93.5 dyn·s·cm-5; 95% CI -156.8 to -30.3; p=0.006). The changes in cardiac index (p<0.001) and Borg dyspnoea scale score (p=0.036) were also significantly improved over placebo. 6MWD and WHO functional class were not significantly improved. The common adverse events in the selexipag group corresponded to those generally observed following administration of a prostacyclin analogue.
Conclusion: Selexipag significantly improved PVR and other haemodynamic variables in patients with CTEPH, although exercise capacity remained unchanged. Further large-scale investigation is necessary to prove the role of selexipag in CTEPH.
Copyright ©The authors 2022.
Conflict of interest statement
Conflict of interest: Nippon Shinyaku Co., Ltd, provided grants for this study group. T. Ogo reports personal fees from Nippon Shinyaku Co., Ltd, during the conduct of the study; personal fees from Janssen Pharmaceutical K.K., Bayer Yakuhin, Ltd, Nippon Shinyaku Co., Ltd, GlaxoSmithKline K.K., Pfizer Japan Inc., and Mochida Pharmaceutical Co., Ltd, outside the submitted work. H. Shimokawahara reports grants from Kaneka Corporation, Bayer Taiwan Co., Ltd, Bayer Yakuhin, Ltd, Daiichi Sankyo Company, Ltd, Japan Lifeline Co., Ltd, Actelion Pharmaceuticals Ltd, Pfizer Inc., and Mochida Pharmaceutical Co., Ltd, outside the submitted work. H. Kinoshita reports grants and personal fees from Nippon Shinyaku Co., Ltd, during the conduct of the study; personal fees from Janssen Pharmaceutical K.K., Nippon Shinyaku Co., Ltd, and Bayer Yakuhin, Ltd, outside the submitted work. S. Sakao reports personal fees from Actelion Pharmaceuticals Ltd, Bayer Yakuhin, Ltd, Daiichi Sankyo Company, Ltd, and Pfizer Japan Inc., grants from the Ministry of Health, Labour, and Welfare of Japan (number 27280401), and Grant-in-Aid for Scientific Research B from the Japan Society for the Promotion of Science (JSPS) (number JP18H03664), outside the submitted work. K. Abe reports grants from Mochida Pharmaceutical Co., Ltd, and Daiichi Sankyo Healthcare Co., Ltd, outside the submitted work. H. Maki reports grants from Bayer Yakuhin, Ltd, and Mochida Pharmaceutical Co., Ltd, outside the submitted work. T. Sugano reports personal fees from Janssen Pharmaceutical K.K., Bayer Holding Ltd, Mochida Pharmaceutical Co., Ltd, Daiichi Sankyo Company, Ltd, Takeda Pharmaceutical Company Ltd, Amgen Inc., Otsuka Pharmaceutical Co., Ltd, Novartis Pharma K.K., and Nippon Shinyaku Co., Ltd, outside the submitted work. I. Tsujino reports grants from Actelion Pharmaceuticals Japan Ltd, Mochida Pharmaceutical Co., Ltd, and Nippon Boehringer Ingelheim Co., Ltd, personal fees from Bayer Yakuhin, Ltd, Janssen Pharmaceutical K.K., Pfizer Japan Inc., and Nippon Shinyaku Co., Ltd, outside the submitted work. N. Tanabe reports personal fees from Nippon Shinyaku Co., Ltd, during the conduct of the study; personal fees from Nippon Shinyaku Co., Ltd, Bayer AG, and Janssen Pharmaceutical K.K., outside the submitted work. K. Tatsumi reports personal fees from Nippon Shinyaku Co., Ltd, Janssen Pharmaceutical K.K., and Actelion Pharmaceuticals Ltd, during the conduct of the study. S. Matoba, H. Motoki, N. Takama, J. Ako, Y. Ikeda, S. Joho, T. Saeki and K. Yoshioka, have no conflicts of interest outside the submitted work. N. Shiota, S. Tanaka and C. Yamamoto are employees of Nippon Shinyaku Co., Ltd.
Figures



Comment in
-
Selexipag for inoperable CTEPH: why meeting a primary endpoint simply isn't enough.Eur Respir J. 2022 Jul 7;60(1):2200581. doi: 10.1183/13993003.00581-2022. Print 2022 Jul. Eur Respir J. 2022. PMID: 35798370 No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials