

Bone defect map of the true acetabulum in hip dysplasia (Crowe type II and III) based on three-dimensional image reconstruction analysis
- PMID: 34824356
- PMCID: PMC8617136
- DOI: 10.1038/s41598-021-02448-z
Bone defect map of the true acetabulum in hip dysplasia (Crowe type II and III) based on three-dimensional image reconstruction analysis
Abstract
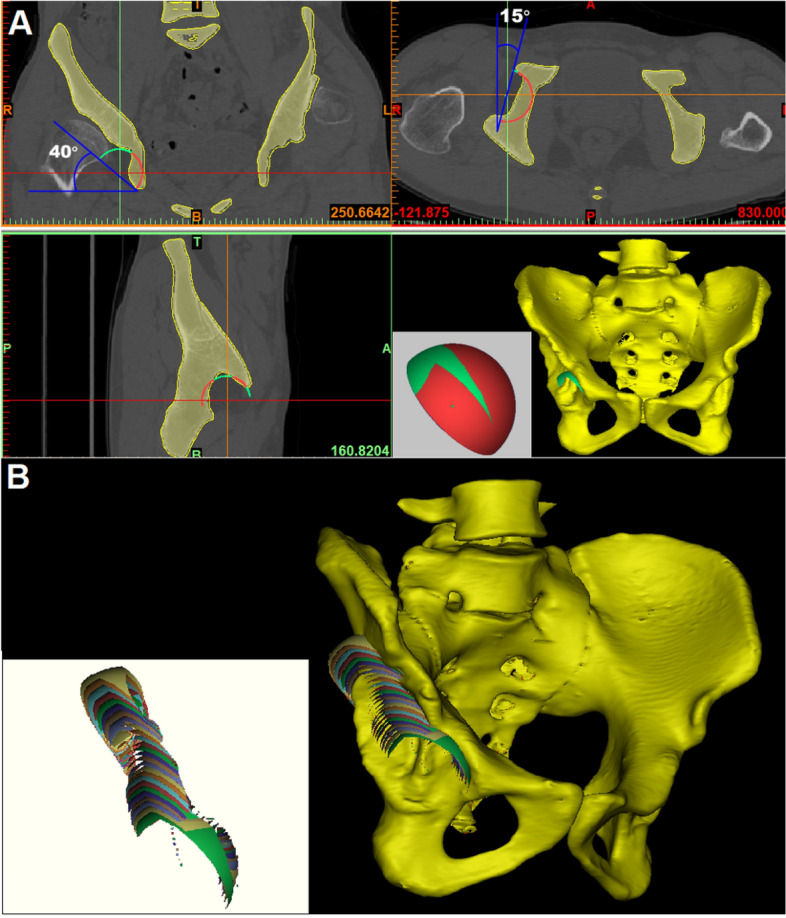
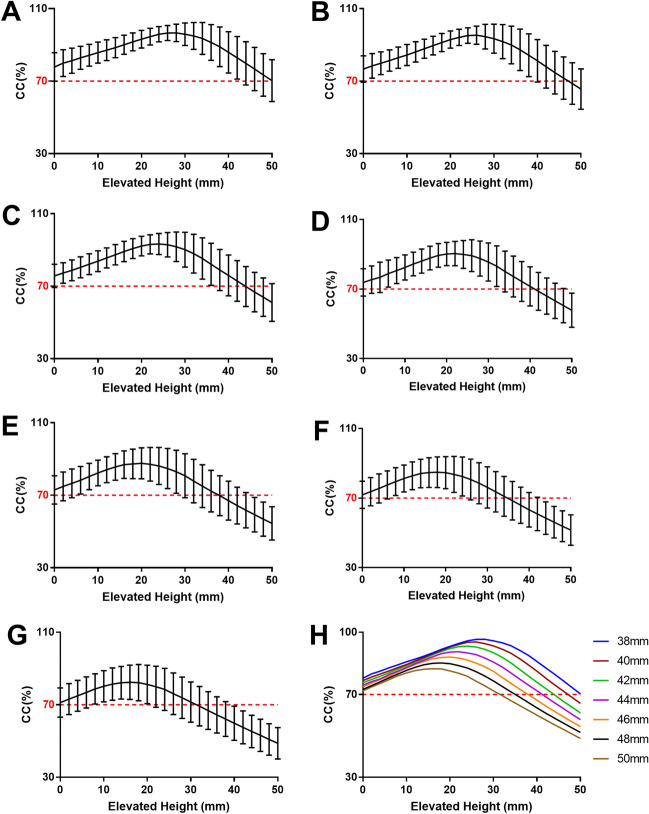
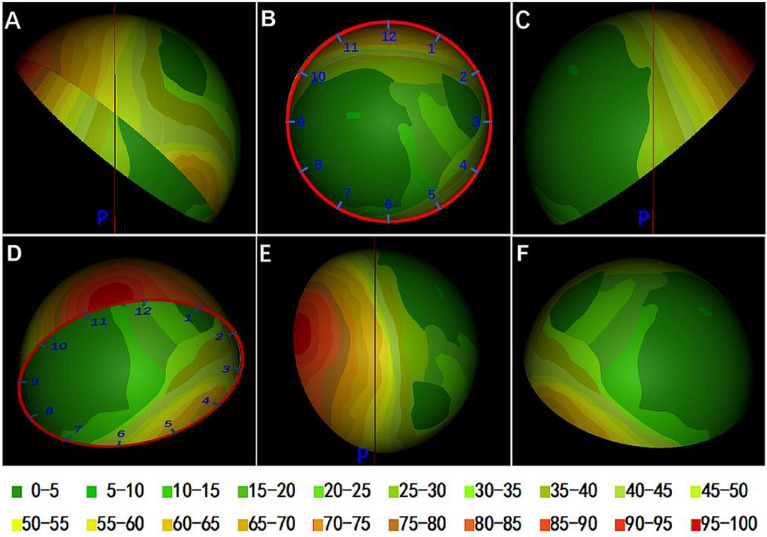
The high hip center technique (HHC) is considered to be feasible for acetabular reconstruction in patients with DDH, but there is little in-depth study of its specific impact on Crowe type II and III DDH. The purpose of this study was to simultaneously analyze the effect of HHC on bone coverage of the cup (CC) in the acetabular reconstruction of type II and III DDH patients and to propose a map of acetabular bone defects from the perspective of the cup. Forty-nine hip CT data of 39 patients with DDH (Crowe type II and III) were collected to simulate acetabular reconstruction by cup models of different sizes (diameter 38mm-50 mm, 2 mm increment) with the HHC technique. The frequency distribution was plotted by overlapping the portions of the 44 mm cups that were not covered by the host bone. The mean CC of cups with sizes of 38 mm, 40 mm, 42 mm, 44 mm, 46 mm, 48 mm, and 50 mm at the true acetabula were 77.85%, 76.71%, 75.73%, 74.56%, 73.68%, 72.51%, and 71.75%, respectively, and the maximum CC increments were 21.24%, 21.58%, 20.86%, 20.04%, 18.62%, 17.18%, and 15.42% (P < 0.001), respectively, after the cups were elevated from the true acetabula. The bone defect map shows that 95% of type II and III DDH acetabula had posterosuperior bone defects, and approximately 60% were located outside the force line of the hip joint. Acetabular cups can meet a CC of more than 70% at the true acetabulum, and approximately 60% of Crowe type II and III DDH patients can obtain satisfactory CC at the true acetabulum by using a 44-mm cup without additional operations.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
