

Predictive Ability of European Heart Surgery Risk Assessment System II (EuroSCORE II) and the Society of Thoracic Surgeons (STS) Score for in-Hospital and Medium-Term Mortality of Patients Undergoing Coronary Artery Bypass Grafting
- PMID: 34824547
- PMCID: PMC8610380
- DOI: 10.2147/IJGM.S338819
Predictive Ability of European Heart Surgery Risk Assessment System II (EuroSCORE II) and the Society of Thoracic Surgeons (STS) Score for in-Hospital and Medium-Term Mortality of Patients Undergoing Coronary Artery Bypass Grafting
Abstract
Objective: To evaluate the powers of European Heart Surgery Risk Assessment System II (EuroSCORE II) and the Society of Thoracic Surgeons (STS) score in predicting in-hospital and medium-term mortality of patients undergoing coronary artery bypass grafting (CABG).
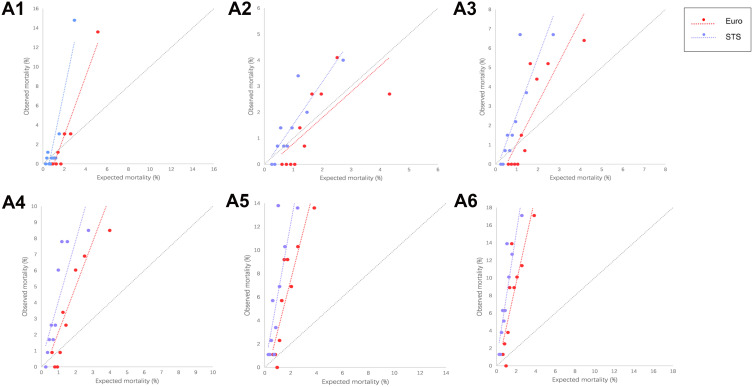
Methods: Totally 1628 Chinese patients were included between January 2000 and January 2018. Their perioperative clinical data were collected and the patients were closely followed up. According to the length of follow-up time, the total cohort was divided into 1-year, 2-year, 3-year, 4-year and 5-year groups. The in-hospital and medium-term risk prediction of EuroSCORE II and STS score were comparatively assessed by calibration, discrimination, decision curve analysis (DCA), net reclassification index (NRI), integrated discrimination improvement (IDI) and Bland-Altman analysis.
Results: About 36 (2.21%) patients died during hospitalization. Both EuroSCORE II and STS score performed extremely well in predicting in-hospital mortality (area under curve = 0.900 and 0.879, respectively). However, calibration and discrimination analyses showed gradual decrease when these two risk evaluation systems were used to predict mortality during the follow-up period. At the same time, the predictive ability of EuroSCORE II was better than STS score. DCA curves showed that the performances of the two evaluation systems were roughly equal between the threshold probability of 0% to 20%. The percentage of correct reclassification of EuroSCORE II was 21.64% higher than that of STS score in predicting 2-year postoperative mortality. The IDI index showed that the predictive capabilities of these two systems were roughly equivalent. Bland-Altman analysis showed no significant difference between the values of the two systems.
Conclusion: EuroSCORE II and STS score have excellent predictive powers in predicting in-hospital mortality of patients undergoing CABG. In particular, EuroSCORE II is superior in calibration and discrimination. The prediction efficiency of the two risk evaluation systems is still acceptable for two-year postoperative mortality, but decreases year by year.
Keywords: EuroSCORE II; STS score; coronary artery bypass grafting; in-hospital mortality; medium-term prognosis.
© 2021 Gao et al.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures




References
LinkOut - more resources
Full Text Sources
