

Association Between Psychiatric Comorbidities and Mortality in Epilepsy
- PMID: 34824893
- PMCID: PMC8610550
- DOI: 10.1212/CPJ.0000000000001114
Association Between Psychiatric Comorbidities and Mortality in Epilepsy
Abstract
Objective: To explore the impact of psychiatric comorbidities on all-cause mortality in adults with epilepsy from a cohort of patients admitted for video-EEG monitoring (VEM) over 2 decades.
Methods: A retrospective medical record audit was conducted on 2,709 adults admitted for VEM and diagnosed with epilepsy at 3 Victorian comprehensive epilepsy programs from 1995 to 2015. A total of 1,805 patients were identified in whom the record of a clinical evaluation by a neuropsychiatrist was available, excluding 27 patients who died of a malignant brain tumor known at the time of VEM admission. Epilepsy and lifetime psychiatric diagnoses were determined from consensus opinion of epileptologists and neuropsychiatrists involved in the care of each patient. Mortality and cause of death were determined by linkage to the Australian National Death Index and National Coronial Information System.
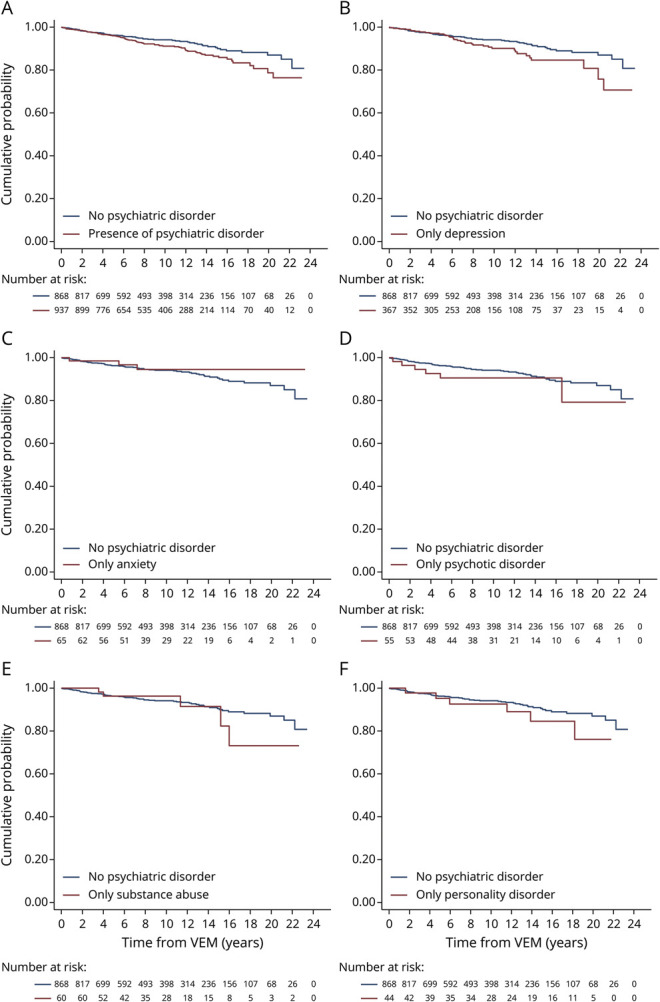
Results: Compared with the general population, mortality was higher in people with epilepsy (PWE) with a psychiatric illness (standardized mortality ratio [SMR] 3.6) and without a psychiatric illness (SMR 2.5). PWE with a psychiatric illness had greater mortality compared with PWE without (hazard ratio 1.41, 95% confidence interval 1.02-1.97) after adjusting for age and sex. No single psychiatric disorder by itself conferred increased mortality in PWE. The distribution of causes of death remained similar between PWE with psychiatric comorbidities and those without.
Conclusion: The presence of comorbid psychiatric disorders in adults with epilepsy is associated with increased mortality, highlighting the importance of identifying and treating psychiatric comorbidities in these patients.
Copyright © 2021 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology.
Figures
References
-
- Hitiris N, Mohanraj R, Norrie J, et al. Mortality in epilepsy. Epilepsy Behav. 2007;10(3):363-376. - PubMed
-
- Nevalainen O, Ansakorpi H, Simola M, et al. Epilepsy-related clinical characteristics and mortality: a systematic review and meta-analysis. Neurology. 2014;83(21):1968-1977. - PubMed
-
- Shankar R, Cox D, Jalihal V, et al. Sudden unexpected death in epilepsy (SUDEP): development of a safety checklist. Seizure. 2013;22(10):812-817. - PubMed
LinkOut - more resources
Full Text Sources