

Mechanisms of oxygenation responses to proning and recruitment in COVID-19 pneumonia
- PMID: 34825929
- PMCID: PMC8617364
- DOI: 10.1007/s00134-021-06562-4
Mechanisms of oxygenation responses to proning and recruitment in COVID-19 pneumonia
Abstract
Purpose: This study aimed at investigating the mechanisms underlying the oxygenation response to proning and recruitment maneuvers in coronavirus disease 2019 (COVID-19) pneumonia.
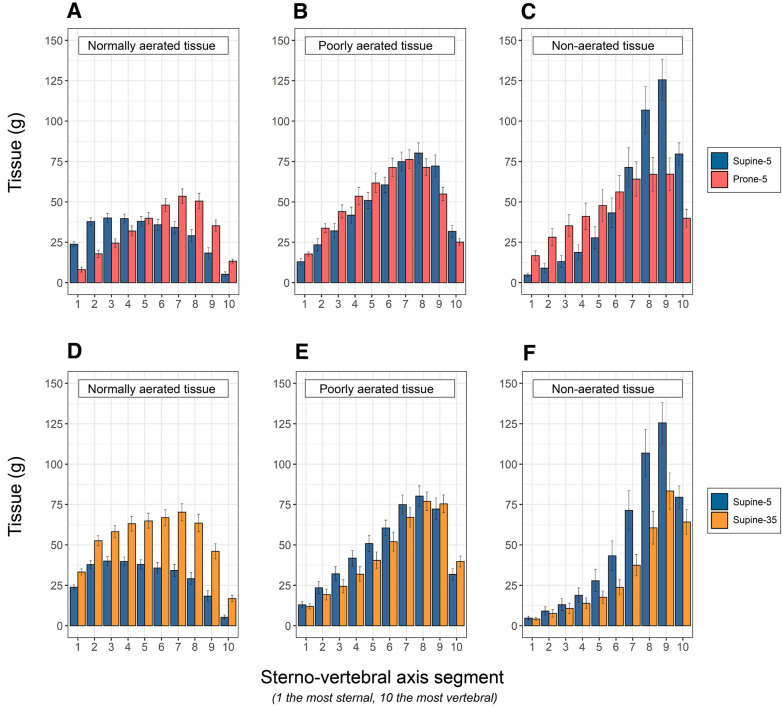
Methods: Twenty-five patients with COVID-19 pneumonia, at variable times since admission (from 1 to 3 weeks), underwent computed tomography (CT) lung scans, gas-exchange and lung-mechanics measurement in supine and prone positions at 5 cmH2O and during recruiting maneuver (supine, 35 cmH2O). Within the non-aerated tissue, we differentiated the atelectatic and consolidated tissue (recruitable and non-recruitable at 35 cmH2O of airway pressure). Positive/negative response to proning/recruitment was defined as increase/decrease of PaO2/FiO2. Apparent perfusion ratio was computed as venous admixture/non aerated tissue fraction.
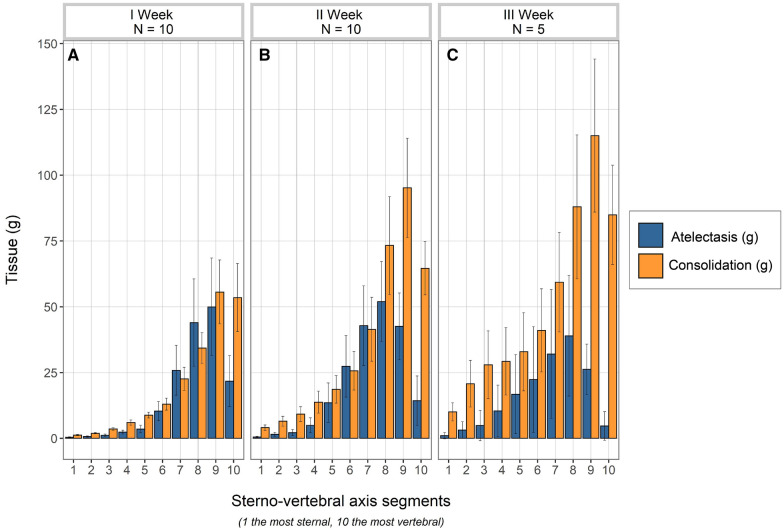
Results: The average values of venous admixture and PaO2/FiO2 ratio were similar in supine-5 and prone-5. However, the PaO2/FiO2 changes (increasing in 65% of the patients and decreasing in 35%, from supine to prone) correlated with the balance between resolution of dorsal atelectasis and formation of ventral atelectasis (p = 0.002). Dorsal consolidated tissue determined this balance, being inversely related with dorsal recruitment (p = 0.012). From supine-5 to supine-35, the apparent perfusion ratio increased from 1.38 ± 0.71 to 2.15 ± 1.15 (p = 0.004) while PaO2/FiO2 ratio increased in 52% and decreased in 48% of patients. Non-responders had consolidated tissue fraction of 0.27 ± 0.1 vs. 0.18 ± 0.1 in the responding cohort (p = 0.04). Consolidated tissue, PaCO2 and respiratory system elastance were higher in patients assessed late (all p < 0.05), suggesting, all together, "fibrotic-like" changes of the lung over time.
Conclusion: The amount of consolidated tissue was higher in patients assessed during the third week and determined the oxygenation responses following pronation and recruitment maneuvers.
Keywords: ARDS; COVID-19; Lung recruitment; Mechanical ventilation; Prone position.
© 2021. The Author(s).
Conflict of interest statement
The authors have no competing interests to disclose.
Figures
Comment in
-
Effect of proning and recruitment on physio-anatomical variables in COVID-19 pneumonia.Intensive Care Med. 2022 May;48(5):636-637. doi: 10.1007/s00134-022-06627-y. Epub 2022 Jan 21. Intensive Care Med. 2022. PMID: 35061054 Free PMC article. No abstract available.
References
-
- Grasselli G, Tonetti T, Protti A, Langer T, Girardis M, Bellani G, Laffey J, Carrafiello G, Carsana L, Rizzuto C, Zanella A, Scaravilli V, Pizzilli G, Grieco DL, Di Meglio L, de Pascale G, Lanza E, Monteduro F, Zompatori M, Filippini C, Locatelli F, Cecconi M, Fumagalli R, Nava S, Vincent JL, Antonelli M, Slutsky AS, Pesenti A, Ranieri VM, Collaborators Pathophysiology of COVID-19-associated acute respiratory distress syndrome: a multicentre prospective observational study. Lancet Respir Med. 2020;8(12):1201–1208. doi: 10.1016/S2213-2600(20)30370-2. - DOI - PMC - PubMed
-
- Beloncle FM, Pavlovsky B, Desprez C, Fage N, Olivier PY, Asfar P, Richard JC, Mercat A. Recruitability and effect of PEEP in SARS-Cov-2-associated acute respiratory distress syndrome. Ann Intensive Care. 2020;10(1):55. doi: 10.1186/s13613-020-00675-7.PMID:32399901;PMCID:PMC7215140. - DOI - PMC - PubMed
