

End of life in the critically ill patient: evaluation of experience of end of life by caregivers (EOLE study)
- PMID: 34825996
- PMCID: PMC8626545
- DOI: 10.1186/s13613-021-00944-z
End of life in the critically ill patient: evaluation of experience of end of life by caregivers (EOLE study)
Erratum in
-
Correction to: End of life in the critically ill patient: evaluation of experience of end of life by caregivers (EOLE study).Ann Intensive Care. 2021 Dec 29;11(1):186. doi: 10.1186/s13613-021-00973-8. Ann Intensive Care. 2021. PMID: 34964064 Free PMC article. No abstract available.
Abstract
Background: The death rate in intensive care units (ICUs) can reach 20%. More than half occurs after a decision of care withholding/withdrawal. We aimed at describing and evaluating the experience of ICU physicians and nurses involved in the end-of-life (EOL) procedure. Primary objective was the evaluation of the experience of EOL assessed by the CAESAR questionnaire. Secondary objectives were to describe factors associated with a low or high score and to examine the association between Numeric Analogic Scale and quality of EOL.
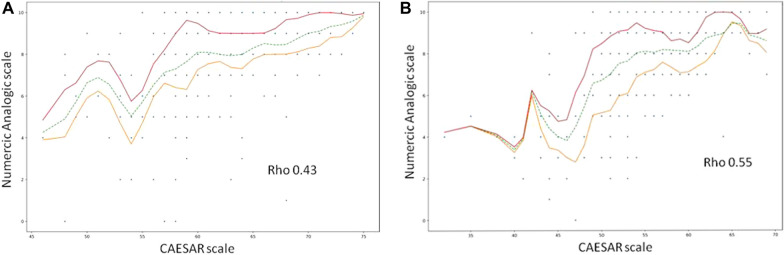
Methods: Consecutive adult patients deceased in 52 ICUs were included between April and June 2018. Characteristics of patients and caregivers, therapeutics and care involved after withdrawal were recorded. CAESAR score included 15 items, rated from 1 (traumatic experience) to 5 (comforting experience). The sum was rated from 15 to 75 (the highest, the best experience). Numeric Analogic Scale was rated from 0 (worst EOL) to 10 (optimal EOL).
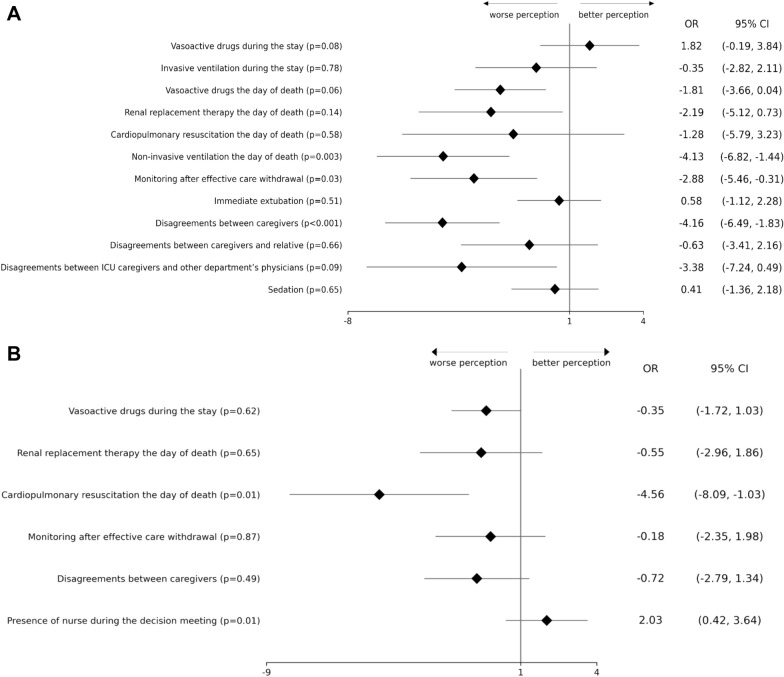
Results: Five hundred and ten patients were included, 403 underwent decision of care withholding/withdrawal, and among them 362 underwent effective care withdrawal. Among the 510 patients, mean CAESAR score was 55/75 (± 6) for nurses and 62/75 (± 5) for physicians (P < 0.001). Mean Numeric Analogic Scale was 8 (± 2) for nurses and 8 (± 2) for physicians (P = 0.06). CAESAR score and Numeric Analogic Scale were significantly but weakly correlated. They were significantly higher for both nurses and physicians if the patient died after a decision of withholding/withdrawal. In multivariable analysis, among the 362 patients with effective care withdrawal, disagreement on the intensity of life support between caregivers, non-invasive ventilation and monitoring and blood tests the day of death were associated with lower score for nurses. For physicians, cardiopulmonary resuscitation the day of death was associated with lower score in multivariable analysis.
Conclusion: Experience of EOL was better in patients with withholding/withdrawal decision as compared to those without. Our results suggest that improvement of nurses' participation in the end-of-life process, as well as less invasive care, would probably improve the experience of EOL for both nurses and physicians. Registration: ClinicalTrial.gov: NCT03392857.
Keywords: Critical care; End of life; Withdrawal treatment; Withholding treatment.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interest.
Figures
References
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
