

Peritoneal malignancy: anatomy, pathophysiology and an update on modern day imaging
- PMID: 34826229
- PMCID: PMC9153709
- DOI: 10.1259/bjr.20210217
Peritoneal malignancy: anatomy, pathophysiology and an update on modern day imaging
Abstract
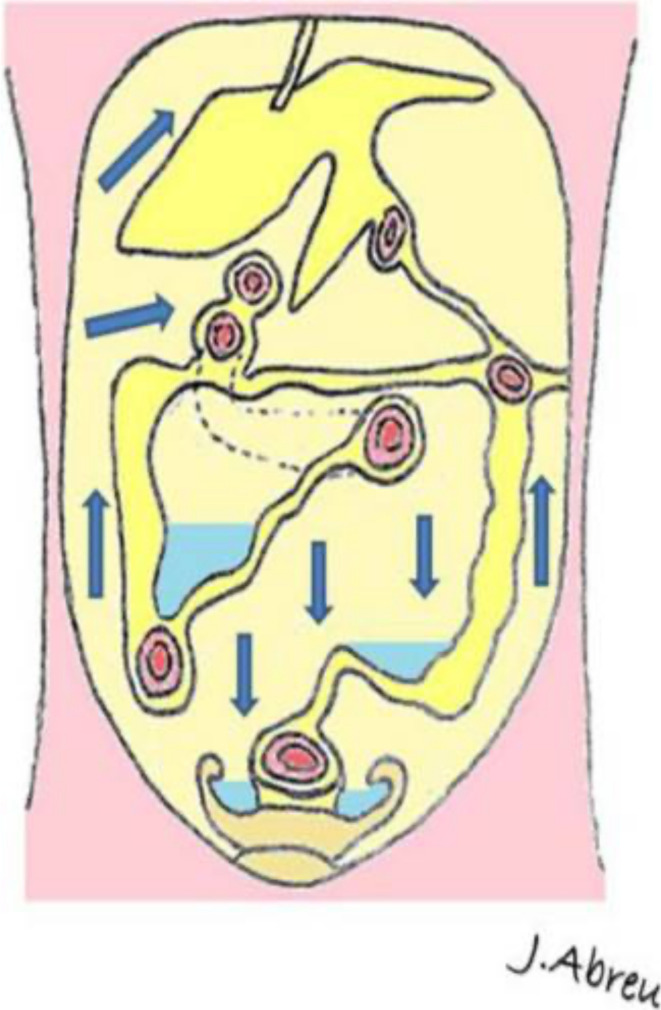
With increasing subspecialised experience in radical cytoreductive surgery and intra-abdominal chemotherapy for peritoneal malignancy, outcomes have improved significantly in selected patients. The surgery and the treatment regimens are radical and therefore correct patient selection is critical. The radiologist plays a central role in this process by estimating, as precisely as possible, the pre-treatment disease burden. Because of the nature of the disease process, accurate staging is not an easy task. Tumour deposits may be very small and in locations where they are very difficult to detect. It must be acknowledged that no form of modern day imaging has the capability of detecting the smallest peritoneal nodules, which may only be visible to direct inspection or histopathological evaluation. Nonetheless, it behoves the radiologist to be as exact and precise as possible in the reporting of this disease process. This is both to select patients who are likely to benefit from radical treatment, and just as importantly, to identify patients who are unlikely to achieve adequate cytoreductive outcomes. In this review, we outline the patterns of spread of disease and the anatomic basis for this, as well as the essential aspects of reporting abdominal studies in this patient group. We provide an evidence-based update on the relative strengths and limitations of our available multimodality imaging techniques namely CT, MRI and positron emission tomography/CT.
Figures

References
-
- Sadeghi B, Arvieux C, Glehen O, Beaujard AC, Rivoire M, Baulieux J, et al. . Peritoneal carcinomatosis from non-gynecologic malignancies: results of the EVOCAPE 1 multicentric prospective study. Cancer 2000; 88: 358–63. doi: 10.1002/(sici)1097-0142(20000115)88:2<358::aid-cncr16>3.0.co;2-o - DOI - PubMed
-
- Verwaal VJ, van Ruth S, de Bree E, van Sloothen GW, van Tinteren H, Boot H, et al. . Randomized trial of cytoreduction and hyperthermic intraperitoneal chemotherapy versus systemic chemotherapy and palliative surgery in patients with peritoneal carcinomatosis of colorectal cancer. J Clin Oncol 2003; 21: 3737–43. doi: 10.1200/JCO.2003.04.187 - DOI - PubMed
-
- Verwaal VJ, Bruin S, Boot H, van Slooten G, van Tinteren H. 8-year follow-up of randomized trial: cytoreduction and hyperthermic intraperitoneal chemotherapy versus systemic chemotherapy in patients with peritoneal carcinomatosis of colorectal cancer. Ann Surg Oncol 2008; 15: 2426–32. doi: 10.1245/s10434-008-9966-2 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
