

A Predictive Model for Severe COVID-19 in the Medicare Population: A Tool for Prioritizing Primary and Booster COVID-19 Vaccination
- PMID: 34827181
- PMCID: PMC8614832
- DOI: 10.3390/biology10111185
A Predictive Model for Severe COVID-19 in the Medicare Population: A Tool for Prioritizing Primary and Booster COVID-19 Vaccination
Abstract
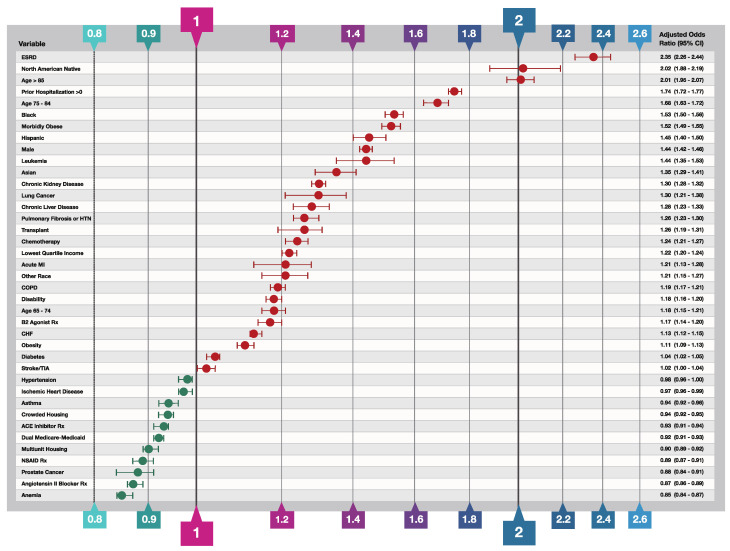
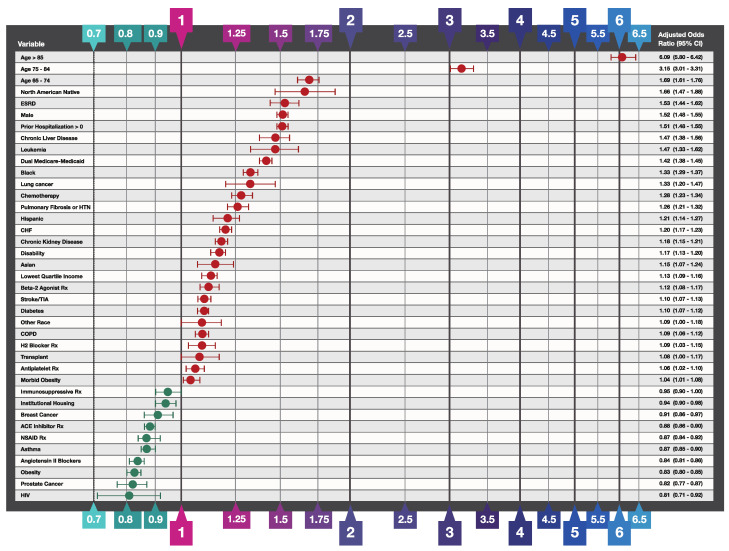
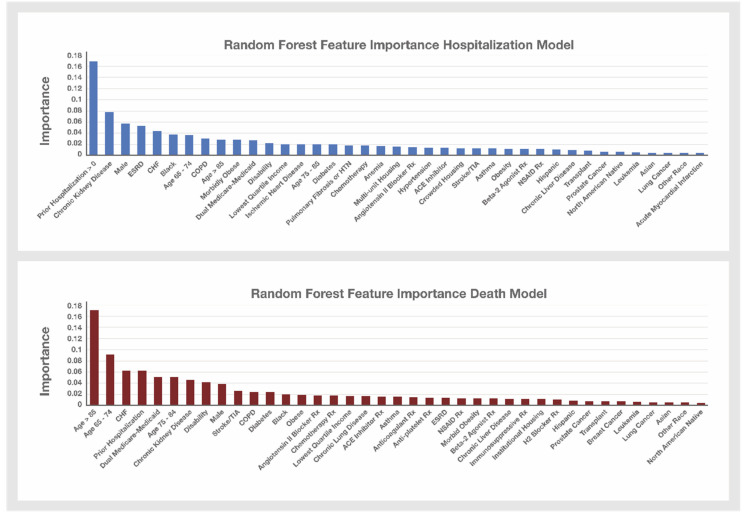
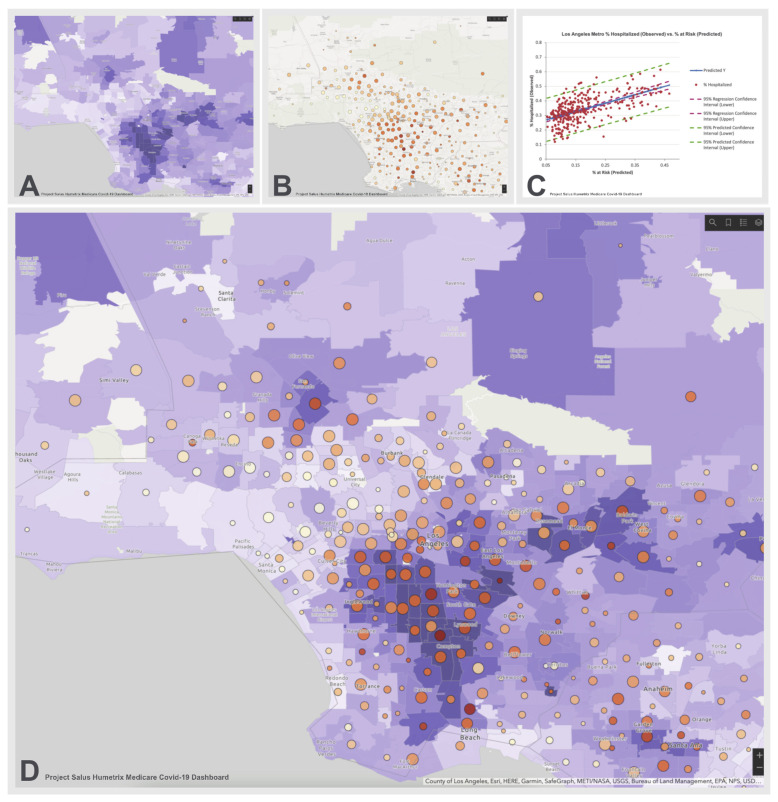
Recommendations for prioritizing COVID-19 vaccination have focused on the elderly at higher risk for severe disease. Existing models for identifying higher-risk individuals lack the needed integration of socio-demographic and clinical risk factors. Using multivariate logistic regression and random forest modeling, we developed a predictive model of severe COVID-19 using clinical data from Medicare claims for 16 million Medicare beneficiaries and socio-economic data from the CDC Social Vulnerability Index. Predicted individual probabilities of COVID-19 hospitalization were then calculated for population risk stratification and vaccine prioritization and mapping. The leading COVID-19 hospitalization risk factors were non-white ethnicity, end-stage renal disease, advanced age, prior hospitalization, leukemia, morbid obesity, chronic kidney disease, lung cancer, chronic liver disease, pulmonary fibrosis or pulmonary hypertension, and chemotherapy. However, previously reported risk factors such as chronic obstructive pulmonary disease and diabetes conferred modest hospitalization risk. Among all social vulnerability factors, residence in a low-income zip code was the only risk factor independently predicting hospitalization. This multifactor risk model and its population risk dashboard can be used to optimize COVID-19 vaccine allocation in the higher-risk Medicare population.
Keywords: COVID-19 booster vaccine; COVID-19 vaccine booster prioritization; COVID-19 vaccine prioritization; Medicare population; risk for severe COVID-19 infection; severe COVID-19 disease; severe COVID-19 risk model.
Conflict of interest statement
Bettina Experton, Adrien Elena, Christopher Hein, Blake Schwendiman and Chris Burrow of Humetrix disclose the following potential conflict of interest: this manuscript reports findings of a study conducted by Humetrix with funding from the Johns Hopkins University Applied Physics Laboratory under a prime contract with the Department of Defense Joint Artificial Intelligence Center. Nicole Lurie, Hassan Tetteh, and Peter Walker have no conflict of interest to disclose. Justin Vincent of Amazon Web Services (AWS), discloses the following potential conflict of interest: AWS received fees for professional services rendered by Justin Vincent of AWS for ECS Federal LLC, part of ASGN Federal Incorporated, under a prime contract of the Department of Defense Joint Artificial Intelligence Center.
Figures
References
-
- Oliver S. Overview of Vaccine Equity and Prioritization Frameworks ACIP Meeting September 22, 2020. [(accessed on 19 October 2021)];2020 Centers for Disease Control and Prevention ACIP Covid-19 Vaccines Work Group. Available online: https://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2020-09/COVI....
-
- Centers for Disease Control and Prevention COVID-19 Mortality Overview. [(accessed on 20 October 2021)];2021 Available online: https://www.cdc.gov/nchs/covid19/mortality-overview.htm.
-
- Centers for Disease Control and Prevention COVID-19 Information for Specific Groups of People updated April 20, 2021. [(accessed on 19 October 2021)];2021 Available online: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/index.h....
-
- National Academies of Sciences, Engineering, and Medicine National Academies Release Framework for Equitable Allocation of a COVID-19 Vaccine for Adoption by HHS, State, Tribal, Local, and Territorial Authorities. 2020. [(accessed on 19 October 2021)]. ScienceDaily. Available online: wwwsciencedaily.com/releases/2020/10/201002111729.htm.
-
- Centers for Disease Control and Prevention CDC SVI 2018 Documentation. [(accessed on 19 October 2021)];2021 Available online: https://svi.cdc.gov/Documents/Data/2018_SVI_Data/SVI2018Documentation.pdf.
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
