

Understanding Parinaud's Syndrome
- PMID: 34827468
- PMCID: PMC8615667
- DOI: 10.3390/brainsci11111469
Understanding Parinaud's Syndrome
Abstract
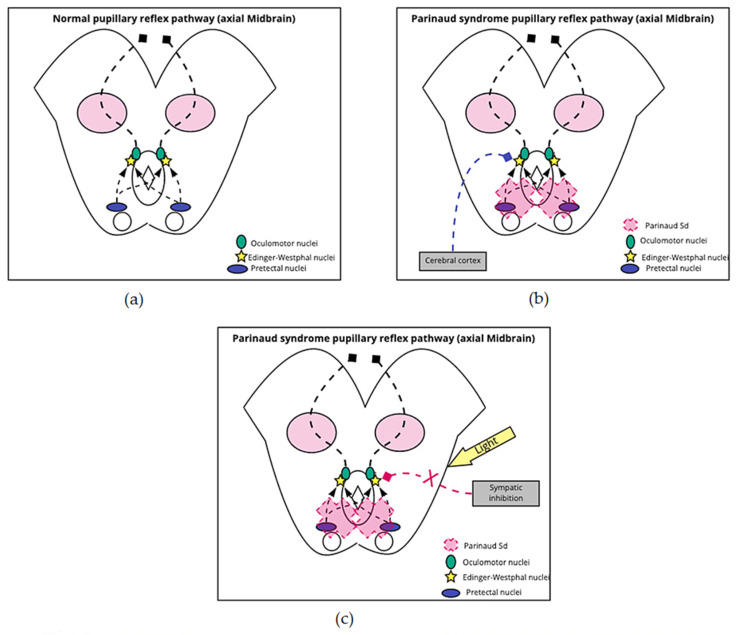
Parinaud's syndrome involves dysfunction of the structures of the dorsal midbrain. We investigated the pathophysiology related to the signs and symptoms to better understand the symptoms of Parinaud's syndrome: diplopia, blurred vision, visual field defects, ptosis, squint, and ataxia, and Parinaud's main signs of upward gaze paralysis, upper eyelid retraction, convergence retraction nystagmus (CRN), and pseudo-Argyll Robertson pupils. In upward gaze palsy, three structures are disrupted: the rostral interstitial nucleus of the medial longitudinal fasciculus (riMLF), interstitial nucleus of Cajal (iNC), and the posterior commissure. In CRN, there is a continuous discharge of the medial rectus muscle because of the lack of inhibition of supranuclear fibers. In Collier's sign, the posterior commissure and the iNC are mainly involved. In the vicinity of the iNC, there are two essential groups of cells, the M-group cells and central caudal nuclear (CCN) group cells, which are important for vertical gaze, and eyelid control. Overstimulation of the M group of cells and increased firing rate of the CCN group causing eyelid retraction. External compression of the posterior commissure, and pretectal area causes pseudo-Argyll Robertson pupils. Pseudo-Argyll Robertson pupils constrict to accommodation and have a slight response to light (miosis) as opposed to Argyll Robertson pupils were there is no response to a light stimulus. In Parinaud's syndrome patients conserve a slight response to light because an additional pathway to a pupillary light response that involves attention to a conscious bright/dark stimulus. Diplopia is mainly due to involvement of the trochlear nerve (IVth cranial nerve. Blurry vision is related to accommodation problems, while the visual field defects are a consequence of chronic papilledema that causes optic neuropathy. Ptosis in Parinaud's syndrome is caused by damage to the oculomotor nerve, mainly the levator palpebrae portion. We did not find a reasonable explanation for squint. Finally, ataxia is caused by compression of the superior cerebellar peduncle.
Keywords: collier sign; midbrain; neurology; parinaud; pseudo argyll robertson pupil.
Conflict of interest statement
The authors declare no conflict of interest.
Figures


References
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
