

Heart Rate Variability in Insulo-Opercular Epilepsy
- PMID: 34827504
- PMCID: PMC8615554
- DOI: 10.3390/brainsci11111505
Heart Rate Variability in Insulo-Opercular Epilepsy
Abstract
Background: We aimed to evaluate heart rate variability (HRV) changes in insulo-opercular epilepsy (IOE) and after insulo-opercular surgery.
Methods: We analyzed 5-min resting HRV of IOE patients before and after surgery. Patients' SUDEP-7 risk inventory scores were also calculated. Results were compared with age- and sex-matched patients with temporal lobe epilepsy (TLE) and healthy individuals.
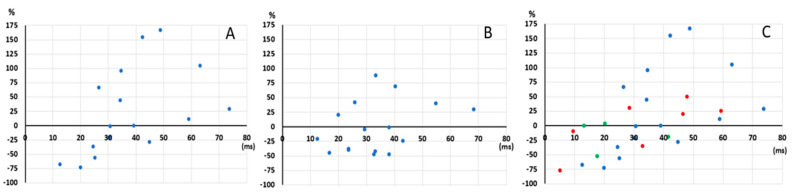
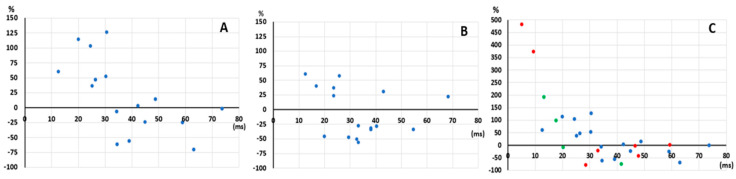
Results: There were no differences in HRV measurements between IOE, TLE, and healthy control groups (and within each IOE group and TLE group) in preoperative and postoperative periods. In IOE patients, the SUDEP-7 score was positively correlated with pNN50 (percentage of successive RR intervals that differ by more than 50 ms) (p = 0.008) and RMSSD (root mean square of successive RR interval differences) (p = 0.019). We stratified IOE patients into those whose preoperative RMSSD values were below (Group 1a = 7) versus above (Group 1b = 9) a cut-off threshold of 31 ms (median value of a healthy population from a previous study). In group 1a, all HRV values significantly increased after surgery. In group 1b, time-domain parameters significantly decreased postoperatively.
Conclusions: Our results suggest that in IOE, HRV may be either decreased in parasympathetic tone or increased globally in both sympathetic and parasympathetic tones. We found no evidence that insulo-opercular surgeries lead to major autonomic dysfunction when a good seizure outcome is reached. The increase in parasympathetic tone observed preoperatively may be of clinical concern, as it was positively correlated with the SUDEP-7 score.
Keywords: cardiac autonomic dysfunction; heart rate variability; insulo-opercular epilepsy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Zerouali Y., Ghaziri J., Nguyen D.K. Multimodal investigation of epileptic networks: The case of insular cortex epilepsy. Prog. Brain Res. 2016;226:1–33. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
