

Automated Analysis of the Two-Minute Walk Test in Clinical Practice Using Accelerometer Data
- PMID: 34827506
- PMCID: PMC8615930
- DOI: 10.3390/brainsci11111507
Automated Analysis of the Two-Minute Walk Test in Clinical Practice Using Accelerometer Data
Abstract
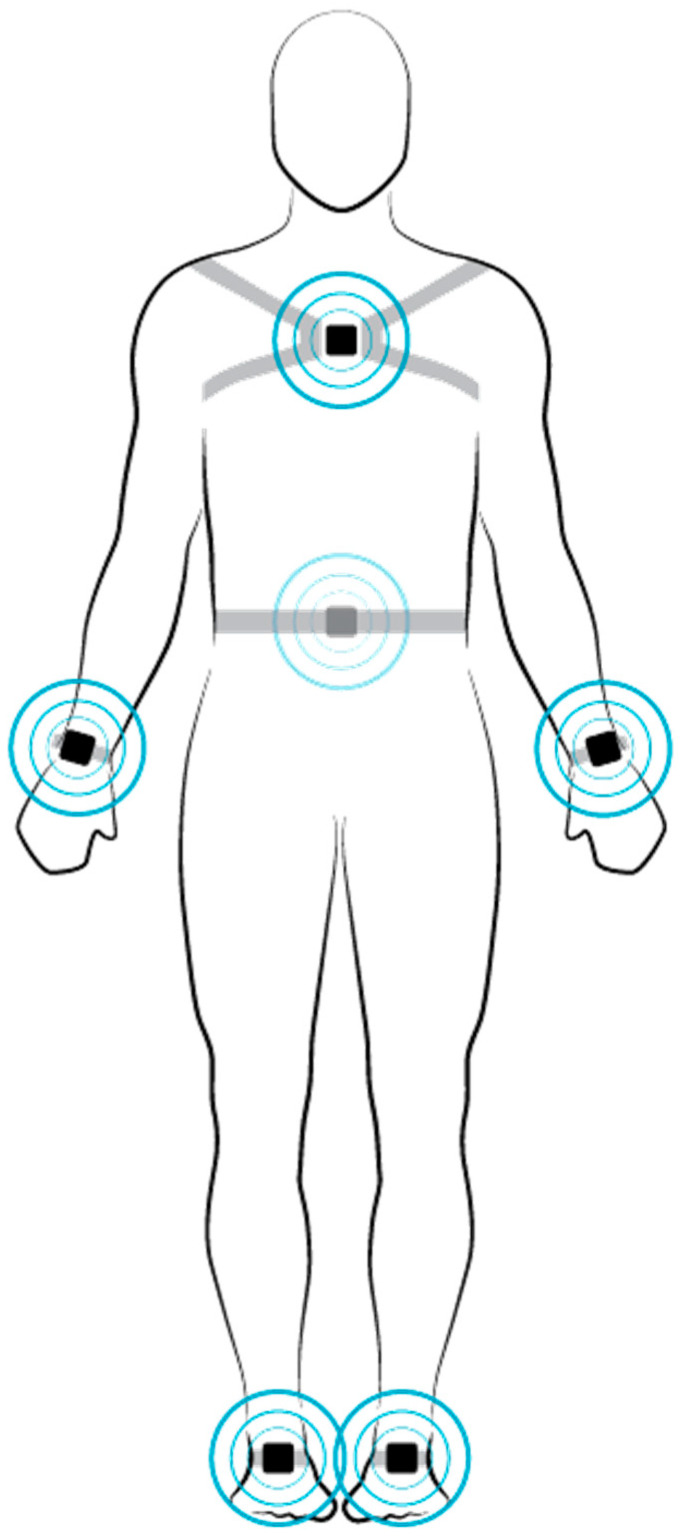
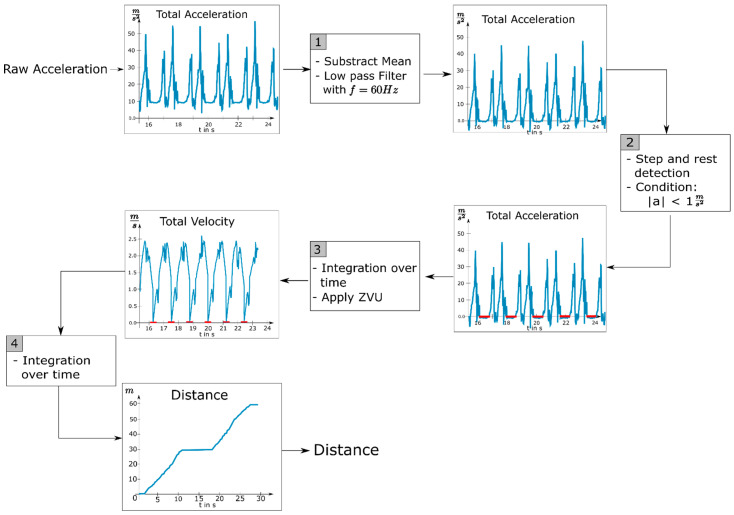
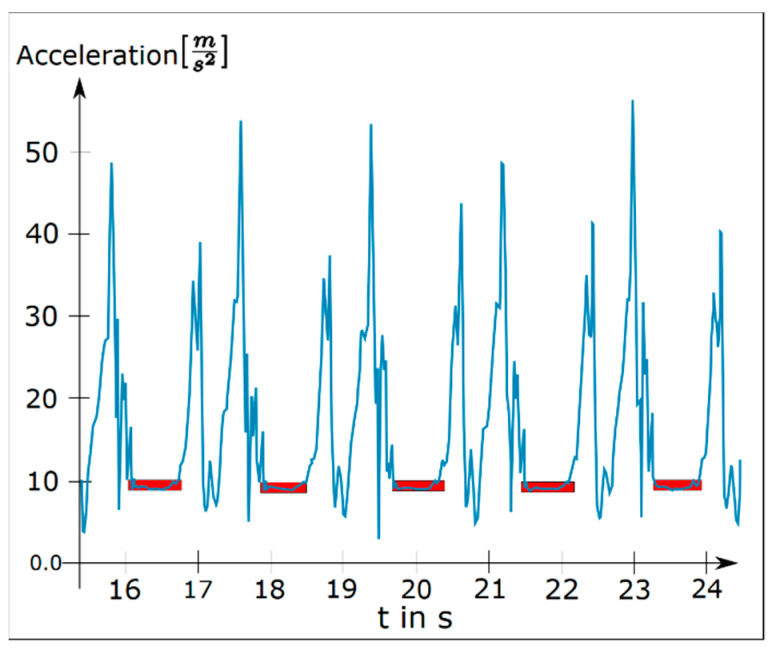
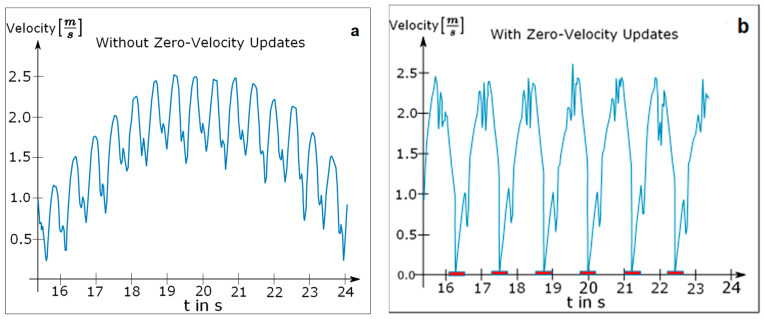
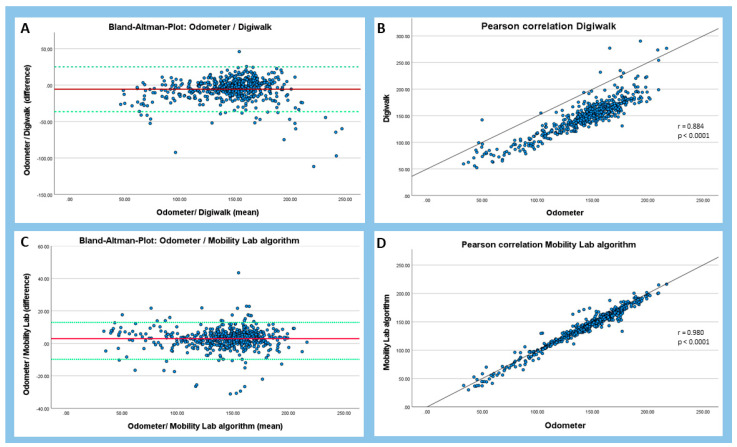
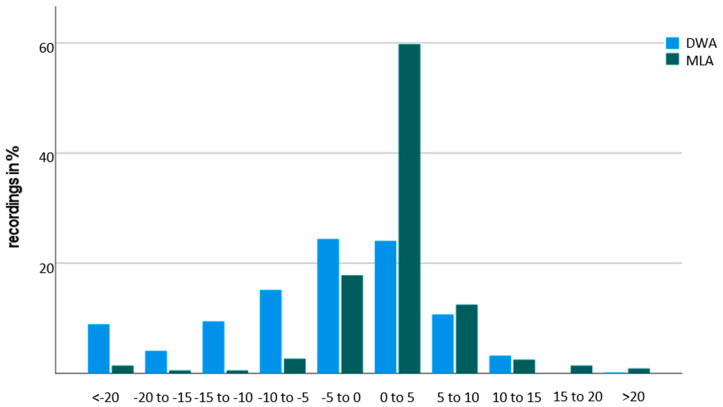
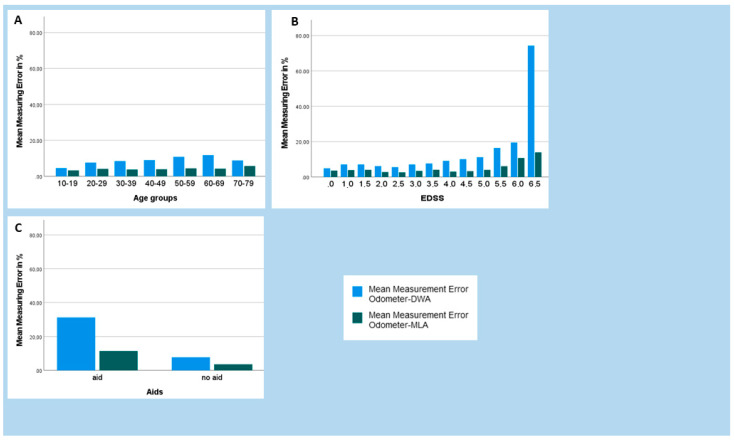
One of the core problems for people with multiple sclerosis (pwMS) is the impairment of their ability to walk, which can be severely restrictive in everyday life. Therefore, monitoring of ambulatory function is of great importance to be able to effectively counteract disease progression. An extensive gait analysis, such as the Dresden protocol for multidimensional walking assessment, covers several facets of walking impairment including a 2-min walk test, in which the distance taken by the patient in two minutes is measured by an odometer. Using this approach, it is questionable how precise the measuring methods are at recording the distance traveled. In this project, we investigate whether the current measurement can be replaced by a digital measurement method based on accelerometers (six Opal sensors from the Mobility Lab system) that are attached to the patient's body. We developed two algorithms using these data and compared the validity of these approaches using the results from 2-min walk tests from 562 pwMS that were collected with a gold-standard odometer. In 48.4% of pwMS, we detected an average relative measurement error of less than 5%, while results from 25.8% of the pwMS showed a relative measurement error of up to 10%. The algorithm had difficulties correctly calculating the walking distances in another 25.8% of pwMS; these results showed a measurement error of more than 20%. A main reason for this moderate performance was the variety of pathologically altered gait patterns in pwMS that may complicate the step detection. Overall, both algorithms achieved favorable levels of agreement (r = 0.884 and r = 0.980) with the odometer. Finally, we present suggestions for improvement of the measurement system to be implemented in the future.
Keywords: digital tools and applications; gait analysis; mobility; multiple sclerosis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
Miscellaneous
